Childhood Pneumonia
Pneumonia is the most common cause of childhood illness. Radiographic interpretation is mainly based on technique. Films are best exposed to maximal inspiration with quiet breathing. Films made in expiration or with the patient rotated may lead to an erroneous diagnosis of pneumonia. The presence of a prominent thymus in an infant, breast buds in the pubescent teenager, or a long hair braid in a child can simulate pneumonia. Also, obstructive airway problems are an important component of childhood nonbacterial respiratory infections. Inflammatory edema, debris & mucus have profound obstructive effects upon small airways in babies. Also, the collateral air pathways are not as well developed. Thus, obstructive overinflation & atelectasis frequently accompany pulmonary infection.
Lobar Pneumonia & Bronchopneumonia
| Lobar pneumonia | Bronchopneumonia |
| It is seen as uniform, homogenous, nonsegmental consolidation |
It is initially patchy and later distributed along the airways-thus it is segmental & non-homogenous. |
| Unifocal in distribution | Multifocal in distribution |
| Mainly involves distal airspaces & spares distal airways | Airways are affected by bronchiolitis. Inflammatory involvement of airways leads to obstruction, atelectasis & occasionally pneumatocele
|
| Air bronchogram is seen | Air bronchogram is not seen |
| Airways are patent so there is no volume loss | Volume Loss is seen |
| Commonly seen with streptococcal pneumonia | Commonly seen with Staphylococcal aureus pneumonia |
Pneumonia - Radiological Features
Though it is difficult to evaluate the organism causing pneumonia, some typical radiological features may suggest the likely etiology:
- Lobar or segmental consolidation & atelectasis are more typical of bacterial infection whereas hyperinflation, bilateral patchy/streaky densities, peribronchial thickening are suggestive of non-bacterial diseases.
- Pneumonia & pleural fluid in a child less than one year indicate staphylococcal infection.
- Hilar/mediastinal lymphadenopathy in conjunction with pulmonary consolidation suggests pulmonary tuberculosis, histoplasmosis, fungal infections.
- Pneumatoceles & classical bronchopneumonia pattern is suggestive of staphylococcal aureus
- Diffuse air trapping with hyperinflation & streaky densities radiating from hila is commonly seen with RSV infection.
- The complete radiographic clearing is the rule in viral infection.
Collapse
Signs of collapse can be divided as:
- Lobar: a shift of fissure, crowding of airways, increased opacity.
- Extralobar: hemidiaphragm elevation, mediastinal shift, hilar shift/distortion, compensatory hyperinflation, rib approximation.
Different lobes of collapse show different features
Right upper lobe collapse: opacity in right upper lobe with minor fissure at cephalic position & its lateral aspect is higher than medial. Adjacent mediastinal silhouette is effaced.
Right middle lobe collapse: Blurring of sharp right heart border & on lateral view, a triangular opacity with apex at hilum is seen.
Lingular collapse: Left cardiac border is ill-defined.
Lower lobe collapse: Triangular opacity in lower lobe with base on diaphragm. Hilar depression, hyperinflation of upper lobe are associated features.
Left lower lobe collapse: shows a retrocardiac triangular opacity.
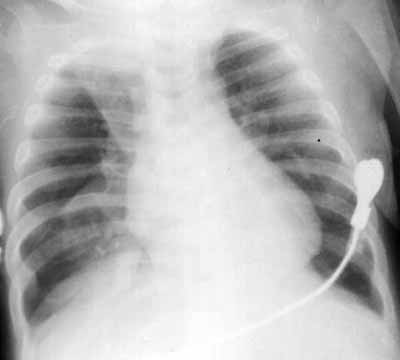
Figure 1: Left lower lobe collapse

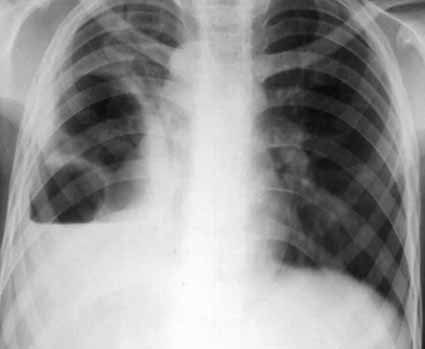
Figure 2: Right middle lobe collapse with minor effusion

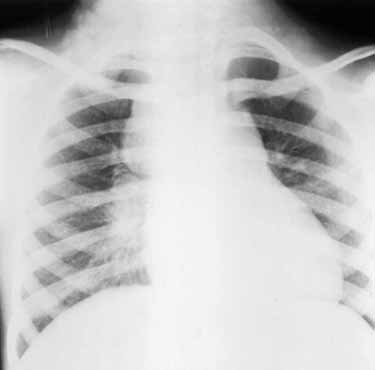
Figure 3: Right upper and lower left lobe collapse
Pleural Effusion
A small amount of free fluid is usually undetectable on chest radiographs. It collects first under the lower lobe - such subpulmonic effusions are detected by lateral decubitus Chest radiographs. Later, there is blunting of posterior & lateral Costophrenic angles (200-500 ml of effusion). Then there is homogenous opacification of the lower chest.
An empyema is radiologically indistinguishable from an effusion on a chest radiograph but should be suspected if pleural effusion is large, delayed in appearance, distributed unusually, or loculated.
The fissural location of free fluid appears sharply marginated, biconvex and has a tail along the fissure.
When in a supine position, pleural effusion appears as a hazy opacity. Associated haziness of diaphragmatic margin, blunting of costophrenic angle, thickening of minor fissure & widening of the paraspinal interface may be apparent.
Figure 4:Encysted effusion in minor fissure

Pneumatocele
Pneumatoceles are defined as thin-walled air containing cavities. In contrast, an abscess has a thick-walled irregular cavity.
There are multiple theories for the formation of pneumatocele:
-
A peribronchial abscess forms that communicate with the airway permitting entry of air into this abscess & when exudate clears, there is the development of a large thin-walled cavity- the pneumatocele. The growth of the pneumatocele occurs because of a ball valve obstruction at the site of the perforation of the airway into the cavity.
- The pneumatocele is formed by the distension of small bronchioles owing to the ball valve effect secondary to bronchial obstruction.
- The current most favored explanation for pneumatoceles is that they are a subpleural collection of air formed by dissection of air from ruptured bronchi or alveoli. The dissection occurs through the interstitium of the lung. On radiographs, pneumatoceles appear as thin-walled air containing lesion - they may show air-fluid levels.
Depending on size, it shows a mass effect/mediastinal shift. They usually appear during the first week of pneumonia & almost always are gone within 6 weeks. The pneumatocele occurs when the child is getting better & its presence does not denote any dire prognostic consequences. Approximately 10% of pneumatocele rupture & cause pneumothorax.
Figure 5: Giant Pneumatocele

Pneumothorax
The diagnosis of even a small quantity of air in the pleural cavity (1 ml) can be made with good quality radiographs. When seen on erect radiographs, pleural air rises to the lung apex & depending on the amount of air, the ipsilateral lung becomes traps radiant. Rarely, expiratory/decubitus films may help to confirm the diagnosis. In the supine position, pleural air rises & collects anteriorly, particularly medially & basally. When pleural space is partly obliterated, a pneumothorax may be loculated. It must be differentiated from other loculated transradiancy like cysts, bullae, pneumatoceles. CT may help in doubtful cases. When fluid accompanies a pneumothorax, the air-fluid level is more eye-catching.
Figure: Pyopneumothorax
Tuberculosis
In a developing country like ours, tuberculosis may have a broad spectrum of manifestations ranging from consolidation, lymphadenopathy, or military shadows. The disease is acquired by inhalation from other infected persons. It may be widespread with meningitis or diffuse pulmonary involvement - may appear radiographically as widespread alveolar infiltrates or as miliary nodules.
The primary complex may manifest a small area of peripheral consolidation (Ghon focus) with a lymph node. The apicoposterior segment of an upper lobe or apical segment of a lower lobe commonly shows consolidation.
Pleural effusion & lymphadenopathy are common associated finding.
Hilar, paratracheal lymph nodes are commonly involved. Though adenopathy is infrequently seen with bacterial/viral infection, histoplasmosis may be a differential diagnosis. Rarely obstructive overinflation of a lobe may be caused by extrinsic bronchial compression by adjacent TB lymph node or endobronchial extension of infection.
Miliary opacities range from 1-2 mm. They are diffuse & of soft tissue density.
Silicosis, berylliosis, sarcoidosis & rarely metastasis cause miliary opacities. Thus, pneumonia with lymphadenopathy or miliary shadows should cause suspicion or tuberculosis.
Figure: Miliary TB

Figure: Pneumonia with hilum enlarged

Figure 9: Paratracheal hilar lymph node
Repeated Non-resolving Pneumonia
Frequent pneumonia in a child should raise suspicion of any congenital anatomical/functional pulmonary abnormality or immunocompromised status. Even after adequate therapy, these pneumonia fail to be cured. Then correlation with serial radiographs is essential.
Repeated RTI is known to occur with heart diseases, cystic fibrosis, asthma, repeated aspirations due to gastro-oesophageal reflux, collagen vascular diseases, etc. Pulmonary sequestration may present as a mass or with high output failure due to (L)-(R) shunt. Sequestration represents a segment of the lung with no developmental connection with the tracheobronchial tree. This is a part of bronchopulmonary foregut malformation. Extralobar sequestrations contained in a separate pleural envelope (60% are seen in children <1 year of age) are more common in a child. Diaphragmatic hernia & congenital heart disease are other associated abnormalities.
Figure 10: Extralobar sequestration
