Introduction
Rickets is a disease caused by a deficiency of Vitamin D leading to bony deformities and hypocalcemia.
Pathophysiological Basis of Radiographic Findings In Rickets
Loss of orderly maturation and mineralization of cartilage cells at the growth plate resulting from Vitamin D deficiency is Rickets. Thus, Rickets is like osteomalacia in a growing skeleton.
Inherent to all rachitic syndromes are osteomalacic changes in portions of the skeleton that contains mineralized bone (Mature bone-both compact & spongy). The skeletal effects are due to a lack of calcification of osteoid. The most obvious change is at metaphysis- where rapid growth is occurring. The first change to appear is a loss of normal zone of provisional calcification adjacent to the metaphysis. This begins as an indistinctness of the metaphyseal margin, progressing to a frayed appearance with a widening of the growth plate, due to lack of calcification of metaphyseal bone. Weight-bearing & stress on the uncalcified bone gives rise to splaying & cupping of metaphysics. A similar but less marked effect occurs in the subperiosteal layer, which may cause a lack of distinctness of cortical margin. Eventually, a generalized reduction in bone density is seen. In the epiphysis - there may be some haziness of cortical margin. Thus, all findings in Rickets occur due to the failure of calcification & abnormal demineralization.
Initial Changes
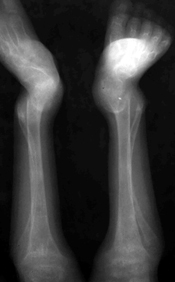
The first changes of rickets appear in rapidly growing distal ends of the ulna & radius (wrist & knee are commonly involved due to more users). Rarefaction of the provisional zone of calcification with the widening of epiphysis-diaphysis distance is first to appear. Following treatment, there is an ossification of the provisional zone of calcification.
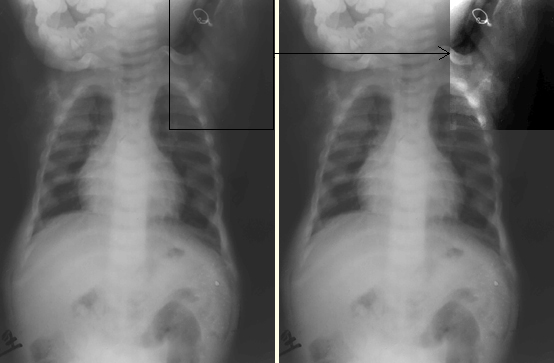
However, early signs of Rickets should be always looked for e.g. On chest X-ray, the humeral head may show certain early radiological changes.
Skull And Spine Changes
Skull changes
- Pronounced calvarial demineralization(Even facial bones are involved)
- Basilar Invagination
- Indistinct sutural margin
- Delayed tooth eruption
- Premature craniostenosis
- Craniotabes
- Calvarial thickening following treatment
Spine changes
- Scoliosis
- Biconcave vertebral bodies
- Triradiate pelvis
Healing Rickets
With treatment, there is a regression of radiological findings seen in Rickets. During a stage of healing, there is extensive periosteal new bone formation as a reflection of ossification occurring along the cornices of diaphyses. Also seen during healing are radiolucent bands at metaphyses of long bones & cupping of metaphyses becomes clearly prominent. As healing progresses remodeling of bowing deformities occur & in the skull characteristic bossing of frontal & parietal bones becomes apparent with premature closure of sutures.
With Renal Tubular acidosis, a peculiar brush border along the metaphysis is seen in the healing phase

Vitamin D Resistant Rickets
Vitamin D Resistant Rickets is found in older children (>30 months of age). The patient is short, stocky & bow legged. Ectopic calcifications & ossification in the axial/appendicular skeleton along with occasional sclerotic changes are among the identifying radiographic features. The bowing of legs & shortening of long bones is more pronounced. Bones are more sclerotic.
Neonatal Rickets
In the first 2 years of life, the incidence of Rickets is 5 to 20%. Neonatal rickets is believed to be of multifactorial origin. Major contributing factors are related to nutrition, immaturity of enzyme systems & iatrogenic/metabolic factors. Premature infants of low birth weight are primarily affected. Bony changes appear around 2 months of age. The most frequent causes of Rickets in patients under 6 months of age also include conditions like Biliary Atresia.
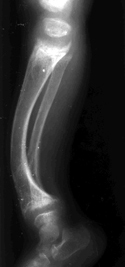
Sequelae Post-Rickets
Complete healing & restoration of the normal structure are the rules in rickets, however, distortion/sclerosis of spongiosa in the affected segment may occur after healing & may remain visible for several years. The cortical thickening of segments of bone involved during the active stage also may persist. Angulation deformities secondary to pathological fractures result in deformities like knock-knee, bow leg, and saber shin.