Reasons for Correction
There are a number of reasons why a testis in an abnormal position must be brought down to the scrotum. The best results are achieved if the surgery is finished by the age of 1 -1 ½ year. The reasons for the operation are:
- When the testis is in an abnormal position its temperature remains higher than in the scrotum by 1-degree Fahrenheit. Just a small difference alters the function of the organ - making of sperms. The process of making sperms in the testis is complicated and involves many stages. It has been proved that the function begins to deteriorate rapidly after 1and a half years if the testis is not in its normal position. By 5 years of age, the tubule producing sperms are reduced by half and the greater the age of the child when testes are brought down, the worse is the function that will be life long. This is directly related to fertility in terms of number and quality of sperms. The chances of such a male to father a child later in life are very much reduced. In fact, even though there may be an undescended testis on only one side, yet, it affects the unction of both sides. It has been shown that even in those boys whose defect has been corrected by the right age still have a 25% chance of infertility.
- In boys with undescended testes, the testis is usually found to be in the inguinal region. In this abnormal position, the boy is more likely to injure the testis while playing, fighting, falling. Due to a direct impact on the testis, it may rupture, cause a blood clot or smash the testis and destroy it. The incidence of trauma to the testis in these boys is far more than that in boys with well-descended testes.
- An undescended testis is not fully down and fixed in position, and hence can move from above downwards, as well as side to side. Since the testis is preceded by its vessels and the vas there can be a twist of the testis on its vessels - called torsion and this can be dangerous. During torsion, the twist can cut off the blood supply to the testis and cause infarction and death of the testis. The testis in such a case will have to be removed permanently. This will affect not only the function of the same side but is also found to adversely affect the opposite side testis function.
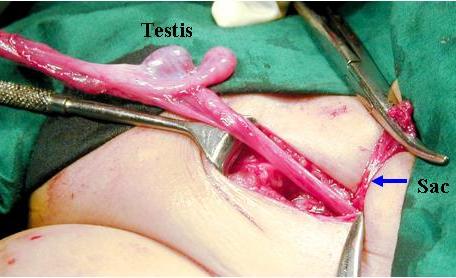
- Associated with undescended testis, there are a high incidence of a hernia almost 60 - 70% cases. Therefore to bring the testis down and to achieve an adequate length, the hernial sac needs to be separated from the cord structures and ligated.
- In later life, the chances of developing cancer of the testis are 20 times higher in a boy with undescended testis, than one with both descended testes. Also higher the initial position of the testis, the more the chances of the malignancy. The importance of this observation is that in cases with treated boys with the testis in the scrotum, in later life one side testis starts growing larger than its counterpart, immediate suspicion is aroused, and a biopsy of that testis needs to be done and if proved positive for cancer, that testis can be removed and other treatment given to control the spread. However, if the testis is in the abdomen, and left untreated, the testis will grow and become cancer and the spread will occur without anyone realizing till it may be too late to treat such a man.
- The last but not the least reason for bringing and fixing the testis in normal position is cosmesis - a boy with no or a single testis is the target of jokes, fun, and teasing. This will make him extremely conscious of the anomaly and have a psychological effect and thus the importance of correction. In cases of absent testis on one side, later - a prosthesis can be inserted after measuring the size of the opposite testis.
Ideal Time for Correction
The ideal age for correction for getting the best results is between 1 to 1½ years of age. The surgery done is called Orchiopexy - that is fixation of the testis in the scrotum and prevent it from going back up where it was. The operation and the approach depending on the site of the testis and the age of the boy. The examination will throw up 2 possibilities - either I am able to feel the testis (called Palpable testis) or I am not able to feel the testis position (called non-palpable testis).
If the testis is felt, no further investigations are required for the testis, and the child can undergo the surgery after routine investigations. This surgery is usually done on a daycare basis - the child comes in the morning, gets operated, and leaves by the evening or night. The surgery lasts for about 1 - 1½ hours. There are 2 incisions in this - one in the inguinal region for the isolation and mobilization of the testis, and the second on the scrotum where the testis is finally brought and sutured to prevent ascent.
Testis found in the inguinal canal

The testis with blood vessels separated from hernia sac
Testis brought down and fixed in scrotum

Hospital Stay
The child does not have to stay in the hospital for more than a day and goes home the same evening or the next morning. In the postoperative period, there will be a swelling both in the inguinal and the scrotal region. This is expected due to the surgery and should not be a cause of worry to the parents of the child. The swelling will gradually decrease within the next few days and the hardening of the incision in the inguinal region will also soften over 3 months. Later, the incision will just be seen but not felt. Usually, antibiotics and anti-inflammatory drugs are given in the immediate post-operative period. The dressing is opened on the 7th postoperative day and left open. Since the sutures used are absorbable, no suture removal is required. The child can start having a bath after the dressing is removed and is allowed full normal activities including sports after 6 weeks of the surgery.
Complications
The problems occur in those boys where I am unable to feel a testis. This could mean that the testis is in the inguinal canal but cannot be felt, the testis could be in the abdomen and hence it cannot be felt, it could have undergone torsion during life and has become small and atrophic hence is not felt, or lastly, the testis could be absent. Differentiating one from the other requires the use of investigations. The first is a simple easily available and non-invasive:
Ultrasonography: This will show the site of the testis clearly if it is in the inguinal region, its dimensions if normal, the previously described operation can be successfully carried out. The testis may be visualized in the inguinal region but may be seen to be small atrophic "possible previous torsion" in such cases during the operation it is advisable to remove the testis rather than keeping a useless testis in the scrotum and let it affect the function of the opposite normal testis.
It may be that the testis is in the abdomen or just inside the canal, but due to technical reasons may not be visualized by Sonography. Hence, non-visualized testis should not be taken as absent testis because time and again I have explored the inguinal region and found a testis of a good size in 8 out of 10 such boys.
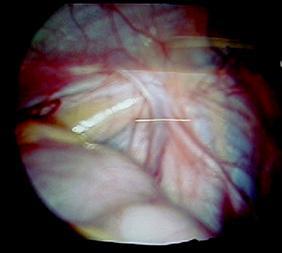
With rapid advances in technology today, I would first do a diagnostic Laparoscopy. This is the introduction of a Pediatric Laparoscope thru a small 5 mm hole made just at the umbilicus and the scope is put inside the abdominal cavity and the side of the missing testis is visualized - three things may be seen 1. The blood vessels and the vas deferens can be seen going into the inguinal canal this means that the testis is present and is in the inguinal canal and can be tackle like previously described and brought down easily. There may be a possibility that the testis is in the inguinal canal but is small and atrophic and hence was not seen on sonography and if so then that testis needs to be removed.
2. The testis may be seen just at the internal ring or higher up. The vessels and the vas are identified and either a one-stage mobilization of the testis or a 2 stage procedure is done to bring the testis down into the scrotum.
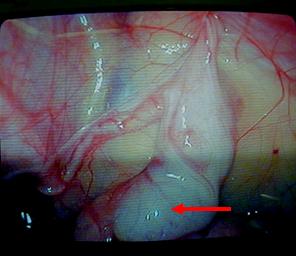
3. In rare cases novas, vessels, or the testis is visualized within the abdomen this is confirmatory of an absent testis. No further procedure is required.
The possible complications of this surgery are damage to the vas or the vessels during handling which can cause rupture or permanent damage to the blood supply or the passage of the sperms into the urethra. This will only be known much later in life after the boy has got married and is unable to conceive a child. Another complication is mechanical - the testis that is brought down to the scrotum is not adequately fixed and can slip back upwards.
Laparoscopic view of vas and vessels
Laparoscopic view of testis in abdomen
Patient Education
This is one condition that has no symptoms but needs to be noticed by the parents. Normally, the testis is formed inside the abdomen below the kidneys (before birth). During the 7th month of pregnancy, the testis is pulled down and in the 9th month. It comes out through the passage and enters the scrotum. At times, due to various reasons - mechanical as well as hormonal, the testis does not fully descend and continues in the abnormal position even after birth. This can occur on one or both sides. The absence of a visible testis should be noticed by the parents early in life. This testis may be felt in the groin or inguinal region, or it may not be felt at all. If the testis can be felt, no other investigations are required; however, if the testis is not palpable, then, it may be inside the abdomen, deep in the inguinal region, or rarely, it may be absent on that side. To find out, there is no foolproof investigation; but sonography to localize the presence and location of a testis is fairly reliable. If no testis is seen, it does not necessarily mean that it is absent but that it could be in a position difficult to detect by sonography. The child must be examined by a Pediatric Surgeon as soon as the parents detect the absence of the testis even if the child is only a few months old. If the child is below 1 year of age, one can wait and see if the testis comes down on its own which is known to happen. However, if the child is above 1 year when seen, then surgery must be planned early.
Absent Testis

Empty scrotum

Why this hurry for this operation?
There are many reasons; the first and most important is the fertility and function of that testis in later life can be permanently affected if the testis remains in the abnormal position for a long time. Lesser is the damage if the correction is done early in life. Abnormality is seen microscopically as early as 2 years of age and progresses rapidly with increasing age without correction. At times, even the opposite normal testis can be affected in function due to the prolonged abnormal position of this side testis. Another reason for surgery is that in 70% of children with this condition, there is an associated hernia that is holding the testis and is preventing it from coming down, and correction of the hernia will automatically free the testis and allow it to come down easily. A third reason is that these non-descended testes midway to their final destination are very mobile and are liable to twist causing torsion of the testis leading to infarction & death of that testis by cutting off of the blood supply. The fourth reason for early surgery is that the likelihood of cancer in that testis which may occur later in life is more in non-descended testes and the longer they are allowed to be in an abnormal position, the higher the chances of undergoing malignant changes.
Thus, these tests need to be brought down and fixed in the scrotum latest by the age of 1-½ years of age to get the best results. If the testis is palpable in the inguinal region, it can be easily brought down in one operation, but those, which are not felt and are in the abdomen, may need one or two operations to be fixed in the scrotum. The operation is done under anesthesia and usually, the child is sent home the same evening or the next day. Healing takes place within 7 days and the boy can resume normal activity in 10 days. Those boys, whose problem is noticed later in life, need to undergo the surgical correction as soon as possible to avoid or minimize the possible complications.