Continued Neurological Damage in HIV Infected Despite Antiretroviral Therapy
Dr Ira Shah, Drishti Tolani
Pediatric HIV Clinic,Department of Pediatrics, B.J.Wadia Hospital for Children, Mumbai, India
Address for Correspondence: Dr Ira Shah, 1/B Saguna, 271/B St Francis Road, Vile Parle (W), Mumbai 400056, India.
Clinical Problem :
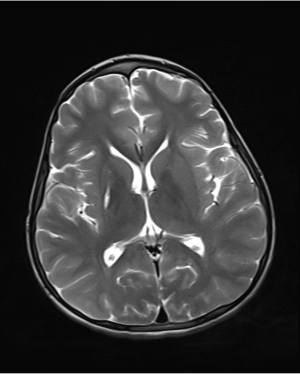
A 13 years old HIV infected boy on ART since 6 years of age presented with progressive increase of involuntary movements of left side of body with increased tone in Sept 2011. He was diagnosed to have left sided dystonia due to infarct in right lentiform nucleus & left cerebellar cortex in April 2004 due to positive antiphospholipid syndrome. (1) At that time he was diagnosed to be HIV infected and was started on Zidovudine (AZT), Lamivudine (3TC) and Nevirapine (NVP) along with aspirin and carbamazepine. His dystonia improved and in 2007 due to epistaxis, his aspirin was omitted. He continued to do well on ART till Feb 2010 when he had CMV retinitis. (2) At that time HIV viral load was undetectable and CD¬4 count was 920 cells/cumm. He was treated with valganciclovir to which his vision improved. His MRI brain in Feb 2010 showed thinning and atrophy of left cerebellar peduncle and left cerebellar hemisphere of unknown etiology. He continued to remain well till July 2011 when parents noticed increased falls due to increase in involuntary movements of left side of body. In Sept 2011, cerebrospinal fluid (CSF) was tested for cytomegalovirus (CMV), Herpes simplex virus (HSV), Epstein barr virus (EBV), HIV proviral DNA and Toxoplasma PCR which were all negative. A repeat MRI was done in Nov 2011 which showed hyper intensities in bilateral cerebellar hemispheres more marked on left side of unknown etiology and right putaminal area of gliosis suggestive of old insult. (Fig 1) His MR angiogram was normal. Subsequently, he became bedridden in Dec 2011 and was hospitalized. His CSF Measles and mumps antibodies were negative. His antiphospholipid antibody (APLA) and anti cardiolipin antibodies were also negative. A brain biopsy from right frontal lobe did not show any viral inclusion bodies. EEG showed generalized slowing. He was continued on ART but he succumbed to his illness.
Figure 1a: T2 weighted image showing hyperintensities in cerebellar hemispheres
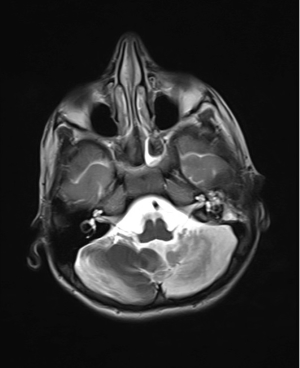
Figure 1b: T2 weighted shows right putaminal area gliosis
|
Why did the child have continued neurological damage inspite of ART?
Discussion :
Neurological complications occur commonly in HIV infected patients and is seen in 20-40% of them. (3) In about 10% patients, the onset of the disease occurs with neurological symptoms. (3) The neurological damage by primary HIV infection is due to activation of microglial cells infected with HIV which in turn spreads the infection to the surrounding tissue. (4) However neurological damage in a case of HIV infection may also be due to opportunistic infections both viral and non viral. (5) There is also an increased incidence of cerebrovascular diseases in children with HIV infection possibly due to vascular immaturity as a contributing factor. (5) Studies have also shown that antiretroviral therapy (ART) and prophylaxis decreases the risk for neurological complications. (5) However continued neurological damage can occur in spite of vigorous antiretroviral therapy. (6) Combination ART effectively decreases the viral load however its poor penetration into the central nervous system (CNS) is responsible for “incomplete protection”. (7) Other than poor access of the drugs into the CNS the other possible hypothetical reasons proposed for the persistence of neurocognitive damages due to HIV even after initiation of ART include failure of antiretroviral agents to reverse neurological damage, chronic systemic immune activation associated with microbial translocation products, sustained CNS inflammation and the possible contribution from aging, amyloid deposition and other co-morbidities. (8) At a study carried out in the National Institute of Health, Bethesda it was observed that 2 out of 11 patients receiving ART with cerebrovascular lesions continued to have persistent viral multiplication. (5) Another study was carried out in Italy to predict the prevalence of neurological damage even after ART and its possible risk factor, it was found that persistent neuropschycolocial effects continued to persist in 62.8% of the patients and thus ART should be initiated as soon as any neurocognitive impairment is diagnosed so as to prevent any irreversible neurological damage. (9)
Thus it is necessary to screen all HIV infected individuals for any neurocognitive diseases and initiate highly active antiretroviral therapy (HAART) at the earliest to prevent any further neurological damage. This is extremely important since HIV associated neurological disorders continue to occur with “less advanced immunosuppression”. (8) Even after HAART has been implemented it is necessary to repeatedly screen the patients for any continued neurological damage. | References : | - Shah I, Chudgar P. Antiphospholipid Syndrome in A Human Immunodeficiency Virus 1-Infected Child. Pediatr Infect Dis J. 2006 ; 25: 185-186
- Shah I, Chilkar S. CMV Retinitis in an HIV infected Child with Undetectable Viral Load. Indian Pediatr. 2010; 47: 893
- Miura Y, Kishida S.Neurological Complications with HIV Infection. Brain Nerve. 2013; 65: 275-81
- Gonzalez-Scarano F, Martin-Garcia J. The neuropathogenesis of AIDS. Nature Reviews Immunology. 2005; 5:69–81
- Manji H, Miller R.The Neurology of HIV Infection. J Neurol Neurosurg Psychiatry. 2004; 75: i29-i35
- Gomes da Silva MM. Neurologic complications of HIV in the HAART era: where are we? Braz J Infect Dis. 2012; 16: 373-378.
- Robertson K, Liner J, Meeker RB. Antiretroviral neurotoxicity. J Neurovirol. 2012; 18:388-99.
- Tan IL, McArthur JC. HIV-associated neurological disorders: a guide to pharmacotherapy. CNS Drugs. 2012; 26: 123-134.
- Tozzi V, Balestra P, Bellagamba R, Corpolongo A, Salvatori MF, Visco-Comandini U, et al. Persistence of neuropsychologic deficits despite long-term highly active antiretroviral therapy in patients with HIV-related neurocognitive impairment: prevalence and risk factors. J Acquir Immune Defic Syndr. 2007; 45: 174-82.
|
| Correct Answers : |  23% 23% |
|
|
|
|
|
|