The diagnosis of pre-symptomatic diseases
Sofia Pimenta1, Sara Soares2, Ana Rita Soares3, Leonilde Machado1
1Department of Pediatrics, Centro Hospitalar Tâmega e Sousa, Portugal, 2Department of Pediatrics, Centro Materno Infantil do Norte, Centro Hospitalar Universitário do Porto, Portugal, 3Medical Genetics Unit, Centro de Genética Médica Doutor Jacinto Magalhães, Centro Hospitalar Universitário do Porto, Portugal
Address for Correspondence: Sofia Pimenta, Avenida do Hospital Padre Américo 210, 4564-007 Penafiel, Portugal.
Email: sofiapimentaa@gmail.com
Keywords: Coffin-Siris Syndrome, pre-symptomatic diseases.
Clinical Problem :
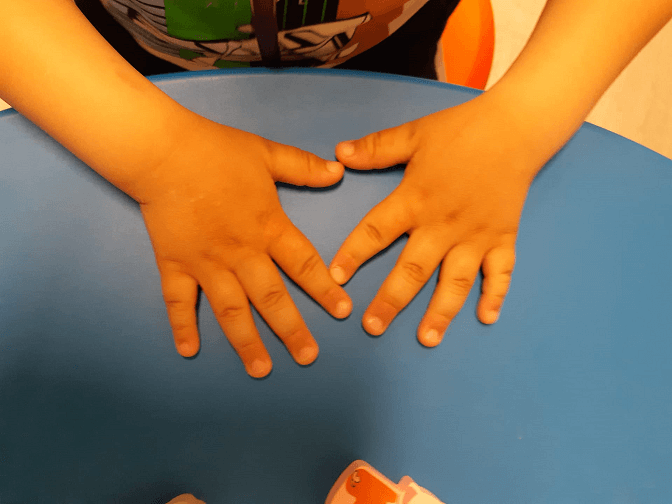
A 4-month-old male child, second child of healthy non-consanguineous parents, with no relevant family history and no prenatal or perinatal complications was referred to a Neurodevelopment clinic due to axial hypotonia, with frequent choking episodes and eating difficulties. On physical examination, the hypotonia was confirmed, with no cephalic control. He had plagiocephaly and few anti-gravity limb movements. He had a systolic murmur. On 2D echocardiography, it was detected to be supravalvular pulmonary stenosis. On the following appointments, hypertelorism and hypoplasia of the nail of the 5th finger were noticed (Figure 1). Meanwhile, with physical therapy support, he started to sit with no support by the age of 9 months, to walk autonomously at the age of 20 months, and said his first words at 24 months old. At 9 months blood tests revealed hypercholesterinemia (254 mg/L) and hypothyroidism (TSH: 5.97 mg/L, free T4: 0.75 mg/L.). He was started on levothyroxine. As first line testing, an array-comparative genomic hybridization (CGH) was performed, revealing a deletion of 1,153 Mbp in the 19p13.2 region, including the genes: 51PR5, ATG4D, MIR1238, KR/1, CDKN2D, APl/1112, SLC44A2, ILF3-AS1, /LF3, QTRTl, DN/1112, M/R638, MIR4748, MIR199Al, MIR6793, TMEDl, C19orf38, CAR/1111, YIPF2, C19orf52, SMARCA4, LDLR, MIR6886, SPC24, KANK2, DOCK6, LOC105372273, ANGPTLB, TSPAN16, RAB3D, TME/111205, CCDC159, PLPPR2, SWSAPl, EPOR, RGL3, CCDC151, PRKCSH, ELAVL3, ZNF653, MIR7974, ECSIT, CNNl, ELOFl, ACP5, ZNF627.
Figure 1. Hypoplastic 5th finger nail.
|
What is the diagnosis?
Discussion :
This deletion includes several genes such as: SMARCA4 - associated with the Coffin-Siris syndrome (CSS) and risk of developing rhabdoid tumours, LDRL - associated with familial hypercholesterolemia, DMN2 - related with autosomal dominant Charcot-Marie-Tooth and with a centronuclear myopathy, and PRKCSH - related with polycystic hepatic disease in adults. After Genetics clinic consultation, the diagnosis of de novo Coffin-Siris syndrome was made, and this patient was also put on follow-up for the risk of the diseases potentially caused by the incidental findings in the genetic study. Coffin-Siris syndrome is a rare genetic disease, characterized by global developmental delay, typical facial dysmorphisms, hirsutism and bilateral aplasia or hypoplasia of the 5 th distal phalange (Figure 1), although other malformations may be found. Several genes ( ARID1A, ARID1B, SMARCA4, SMARCB1, SMARCE1, or SOX11) have been associated with this syndrome, and most of the cases occur as de novo events. 1,2
The use of array-CGH in clinical practice has several implications. Diagnosis can be found for the manifestations in question, but variants of unknown significance or secondary/incidental findings (mainly for pre-symptomatic diseases) can also be detected. The implications of knowing this kind of information have been the subject of much discussion among the scientific and ethical community.
This case portrays a rare situation in which a total genetic deletion of the SMARCA4 gene took place, but there were also deletions of other genes that have clinical significance.
Genetic testing allows to confirm the diagnosis and family counselling. 1 However, when carrying out the genetic study, as in this case, genes were found for pre-symptomatic diseases that are essential for periodic screening, but there may still be no treatments to date.
There is no specific treatment for this illness. When it comes to the increased risk of developing tumours, there are no formal instructions for a routine oncological screening in the individuals with CSS carrying a pathogenic variant on SMARCA4 gene. However, taking into consideration the possible tumour risk, there should be a cautious examination of the patient with the help of complementary means of diagnosis (MRI of the entire body, including the cerebral field) and careful surveillance by a multidisciplinary team. 2,3
Authors Contribution
SP took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript. | References : | - Fleck BJ, Pandya A., Vanner L., Kerkering K, Bodurtha J. Coffin-Siris syndrome: review and presentation of new cases from a questionnaire study. Am J Med Genet. 2001;99:1-7.
- Kosho T, Okamoto N; Coffin-Siris Syndrome International Collaborators. Genotype-phenotype correlation of Coffin-Siris syndrome caused by mutations in SMARCB1, SMARCA4, SMARCE1, and ARID1A. Am J Med Genet C Semin Med Genet. 2014;166C:262-275.
- Del Baldo G, Carta R, Alessi I, Merli P, Agolini E, Rinelli M, et al. Rhabdoid Tumor Predisposition Syndrome: From Clinical Suspicion to General Management. Front Oncol. 2021;11:586288.
|
| Correct Answers : |  100% 100% |
|
|
|
|
|
|