Dr Ira Shah.
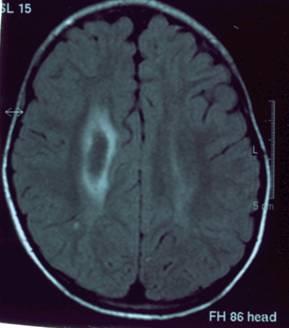
Medical Sciences Department, Pediatric Oncall, Mumbai, India. | | Authors Contribution | A 4 and half years old male child presented with sudden onset left-sided hemiplegia since 2 hours. There was no history of trauma, convulsions, loss of consciousness or bladder-bowel incontinence. The child had no history of jaundice or prolonged antibiotic use. On examination, the child had left supranuclear VII th nerve palsy and (E) left sided weakness (power 2/5) with left-sided hypotonia. The sensory system was normal with no bladder or bowel involvement. Planters on the left side were extensor. His blood pressure was 90/60 mm of Hg and there were no signs of increased intracranial tension. Other systemic examination was normal. He improved within 24 hours and had a complete recovery within 7 days. MRI brain was suggestive of right front parietal bleed that was isointense on T1, & hypointense on T2 suggestive of acute intraparenchymal hematoma (Figure 1). MRA & MRV was normal. Cerebral angiography was normal. His platelet count was normal (2,70,000/cumm) and sickling was negative. Prothrombin time was prolonged (Patient = 19.8 sec., control = 13.9 sec.) and so was partial thromboplastin time (Patient = 107 sec, control = 31.2 sec), which responded to IV Vitamin K. (PT = 14.8 sec, and PTT = 26.8 seconds). His serum fibrinogen, thrombin time, factor XIII levels were also normal. ANA, dsDNA was negative. His liver function tests were also normal. PIVKA could not be done due to unaffordability. Thus a diagnosis of intracranial bleed due to Vitamin K deficiency was made.
Figure 1 : MRI brain showing right front parietal bleed.
 | | | | Discussion | Deficiency of Vitamin K, a fat-soluble vitamin leads to bleeding manifestations.
Types of Vitamin K Deficiency states:
- Early Hemorrhagic Disease of Newborn (Early HDN) - This results in severe and life threatening bleeding (scalp hematoma, intracranial or intra abdominal bleeds) at the time of delivery or during the first 24 hours after birth. It occurs in infants whose mothers have taken drugs such as anti-convulsants, anti-tuberculous drugs, salicylates or coumarin anti-coagulants that affect Vitamin K metabolism.
- Classical HDN - It occurs in 1st week of life and presents as generalized ecchymosis, bleeding from umbilical stump, GI bleed or epistaxis. It is found in healthy term babies who are exclusively breastfed and have not received Vitamin K prophylaxis.
- Late HDN - This occurs between 2-12 weeks of age and may even present up to 1 year of age. It may be idiopathic (occurs between 2-12 weeks of age) or secondary (can occur anytime in the 1st year) due to chronic diarrhea, prolonged use of broad-spectrum antibiotics, cystic fibrosis, biliary atresia, cholestatic hepatitis, celiac disease and chronic warfarin exposure. In idiopathic cases, immaturity of the carboxylase system in the liver has been postulated as the etiological cause. Intracranial bleeds and wide spread ecchymoses are the commonest presenting features. GI or mucosal bleeds or excessive bleeding following IM injections may be infrequent manifestations.
Vitamin K functions
Vitamin K is necessary for production of carboxylated Factor II, VII, IX and X in the coagulation cascade system. Vitamin K deficiency results in non-functional (qualitative) deficiency of above-mentioned factors.
Sources of Vitamin K
Vitamin K occurs in plants and green leafy vegetables as phylloquinone (Vitamin K1). It is also produced as menaquinone (Vitamin K2) endogenously in the gut by bacteria. Menaquinones are not found in significant amount in the liver till about 2 weeks of age. Human milk is a poor source of vitamin K.
Diagnosis of Vitamin K deficiency
Vitamin K deficiency is associated with markedly prolonged partial thromboplastin time (PTT) and Prothrombin time (PT) with normal thrombin time, fibrinogen and platelet count.
Presence of PIVKA (proteins induced In Vitamin K absence - These are non carboxylated forms of Vit K dependent factors) is a highly sensitive & specific marker. PIVKA- II (Non-carboxylated form of prothrombin) is the most sensitive parameter. PT becomes normal as early as 4 hours after administration of vitamin K whereas PIVKA-II has a plasma disappearance time of 70 hours.
Treatment of Vitamin K deficiency
Prevention: A single intramuscular dose (0.5 to 1mg) of vitamin K administered at birth protects against classical HDN and idiopathic late onset HDN up to 3 months of age. Patients receiving TPN should be given biweekly parenteral Vitamin K and those receiving broad-spectrum antibiotics should receive weekly supplementation because of sterilization of the gut. Mothers with "at risk" babies of early HDN should receive prophylactic Vitamin K (20mg orally) daily during last 2 weeks of pregnancy or 10mg orally daily during last 2 months of pregnancy.
Treatment of Vitamin K bleeding manifestation: When deficiency is severe, intramuscular administration of Vitamin K may be associated with hematoma formation and may delay the therapeutic response. Hence IV route is preferred.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Lane PA, Hathaway WE - Vitamin K in infancy. J Pediatrics 1985,106; 351-359. [CrossRef]
- Liebman HA, Furie BC, Furie - Hepatic Vitamin K dependent carboxylation of blood clotting proteins, Hepatology- 1982, 3: 488-494.
- Cornellssen EAM, Kollee IAA, DeAbrell RA et al - Effects of oral and intramuscular Vitamin K prophylaxis on Vitamin K1, PIVKA- II and clotting factors in breast-fed infants. Arch Dis Child 1992, 67: 1250-1254. [CrossRef]
- Deblay MF, Vert P, Andre M et al - Transplacental Vitamin K prevents hemorrhagic diseases of the infant of epileptic mother. Lancet 1982, 1:1247. [CrossRef]
|
| Cite this article as: | | Shah I. VITAMIN K DEFICIENCY. Pediatr Oncall J. 2004;1. |
|