Maryam Hasanzad, Zohreh Mohammad Taheri, Amir Ali Khodayari, Soheila Khalilzadeh.
Pediatric Department, Masih Daneshvari Hospital, Tehran, Iran.
ADDRESS FOR CORRESPONDENCE
Soheila Khalilzadeh, Pediatric Ward, NRITLD, Darabad Ave, Masih Daneshvari Hospital, Tehran, Iran. | | Abstract | | A 12-year old boy was referred to the pediatric pulmonary ward of Masih Daneshvari Hospital due to unexplained chronic cough and presumed diagnosis of miliary pulmonary tuberculosis which was based on a history of exacerbation of 6 month chronic cough and radiological findings of the lungs which showed bilateral multiple micronodular opacities. Physical examination showed a diffuse thyroid gland enlargement and cervical lymphadenopathy. The result of excisional lymph node biopsy revealed papillary thyroid carcinoma. | | | | Introduction | Thyroid cancer, the most common pediatric endocrine neoplasm, represents 1-1.5% of all pediatric malignancies and 5% of malignancies in the head and neck. Only 5% of all thyroid cancers occur in children and adolescents. (1)
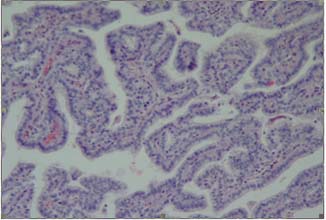
Pediatric thyroid malignancies are usually a well differentiated papillary subtype or the papillary follicular subtype. Children commonly present with advanced disease. At presentation, 70% of patients have extensive regional nodal involvement, and 10-20% of patients have distant metastasis. The lungs are the most common sites of metastasis. Even young patients who have lung metastasis usually do not report pulmonary symptoms (2). | | | | Case Report | A 12 years old boy with complaints of chronic cough since 6 months which was exacerbated during last 2 months was referred to us with presumed diagnosis of miliary tuberculosis due to multiple micronodular opacities in chest radiograph. On examination he wasn't ill or toxic. His weight corresponded to tenth percentile for age. He had significant bilateral cervical lymphadenopathy approximately 2x2 cm. He had thyroid enlargement that was firm and free from surrounding tissues. It measured 6x5 cm on right side and 7x6 cm on the left side. Respiratory system examination revealed coarse crackles at both lung fields. Other systemic examination did not have any abnormality. Laboratory data were normal. Tuberculin test was negative. Three samples of gastric washing for acid fast bacilli were negative. Plain chest x-ray showed diffuse multiple micro nodular opacities in both lungs. High resolution CT-scan (HRCT) revealed diffuse bilateral numerous parenchymal nodules detected through out both lung field (Figure-1). Histopathological examination of cervical node excisional biopsy showed metastatic thyroid papillary carcinoma surrounded by lymphoid tissue. (Figure-2). A subtotal thyroidectomy was done followed 131I ablative therapy and hormone replacement.
Figure 1- Chest CT-scan shows diffuse bilateral numerous parenchymal nodules through out both lung fields
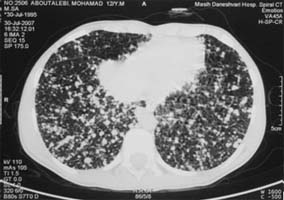
Figure 2- Histopathological examination showed metastatic thyroid papillary carcinoma surrounded by lymphoid tissue
 | | | | Discussion | Carcinoma of thyroid is rare in childhood. A painless nodule in the thyroid or in the neck is the usual first evidence of disease. (3, 4) About 70% of patients have extensive regional nodal involvement, and 10-20% of patients have distant metastasis. (2) Our case also presented with enlarged cervical lymph nodes. Though the lungs are the most common sites of metastasis, pulmonary symptoms have not been yet reported as the first manifestation (2). Lung metastases may develop in 5% to 9% of patients during the course of the disease. (5) In this child, lung metastases appeared as a first manifestation of papillary carcinoma of thyroid but he did not have involvement of any other site, such as bone. Pulmonary metastases carry a very poor prognosis in older patients, but children appear to have much better survival (6, 7). The diagnosis of pulmonary metastasis can be made either by a chest radiograph, or by total body scan (TBS) or by both. Abnormal chest radiograph shows diffuse miliary or "snow storm" pattern or micro-nodular infiltration principally in the basal regions due to the lymphatic spread of the tumor. (3, 6) Our child had miliary mottling in the chest radiograph at presentation which was later confirmed to be metastases by the body scan. Small (<2cm) papillary carcinoma is effectively treated by subtotal thyroidectomy and suppressive doses of thyroid hormones. For larger papillary carcinoma, near total thyroidectomy with excision of the regional lymph nodes appears to be the treatment of choice.
We report this case as an unusual manifestation of thyroid cancer with chronic cough and miliary lung mottling. This case illustrates the need for adequate clinical examination of the thyroid, when chronic cough or miliary mottling is noted in children to avoid misdiagnosis with tuberculosis. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Chaukar DA, Rangarajan V, Nair N, et al. Pediatric thyroid cancer. J Surg Oncol.Nov 1 2005; 92(2)130-3. [CrossRef]
- Yoskovitch A, Laberg JM, Rodd C, et al. Cystic thyroid lesions in children. J Pediatr Surg. Jun 1998; 33(6):866-70. [CrossRef]
- Behrman RE. Thyroid cancer in children. In: Behrman RE, Kliegman RE, Arvin AM, Ed Nelson Text Book of Pediatrics; 18th edn. Philadelphia: W.B. Saunders CO; 2008:1602-03.
- Brisk JS, Van Heerden JA, Mclver B, et al. Papillary thyroid cancer with pulmonary metastases in children: Long-term prognosis. Surgery 2000; 128: 881-87. [CrossRef]
- Hoie J, Steinweg AE, Kullman G, Lindergaard M. Distant metastases in papillary thyroid cancer: A review of 91 patients. Cancer 1988; 61:1-6. [CrossRef]
- Vassilopoulou-sellin R, Kleini MJ, Smith TH, et al. Pulmonary metastases in children and young adults with differentiated thyroid cancer. Cancer 1993; 71: 1348-52. [CrossRef]
- Frankenthaler RA, Vassilopoulou-sellin R, Gangir A, Goerfee H. Lymph node metastases from papillary-follicular thyroid carcinoma in young patients. Am J Surg 1990: 160: 341- 43. [CrossRef]
|
| Cite this article as: | | Hasanzad M, Taheri Z M, Khodayari A A, Khalilzadeh S. Metastatic Lung Lesion In A Child- A Case Report of Thyroid Papillary Carcinoma. Pediatr Oncall J. 2008;5: 121. |
|