Adnan Zafar, Vasudha Jeve.
Department of Paediatrics, Leicester Royal Infirmary, Leicester, UK.
ADDRESS FOR CORRESPONDENCE
Dr Adnan Zafar, Department of Paediatrics, Leicester Royal Infirmary, Infirmary Square, LE15WW, UK.
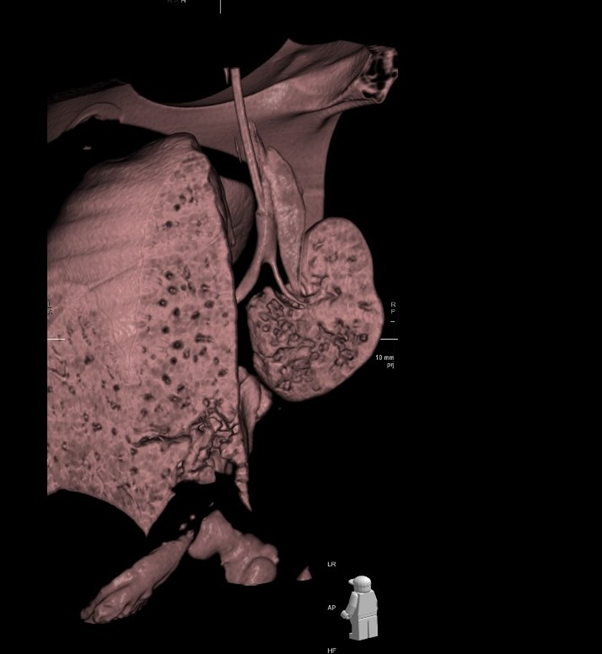
Email: adnan157@gmail.com | A 9 months old infant presented with recurrent lower respiratory tract infections and wheezy episodes. On examination, he had respiratory distress and wheeze, which parents reported to be present for last 3 months. Chest X-ray showed a large right sided homogeneous opacity and shift of the mediastinum to right side (Figure 1). CT thorax showed right pulmonary hypoplasia, with only partial formation of the right upper lobe. The hypoplastic lung was supplied by a small calibre right main pulmonary artery. The azygos vein coursed horizontally into the superior vena cava, suggesting that part of the formed lung was azygos lobe. (Figure 2) There were also segmental anomalies of C7 and T1 vertebra leading to scoliosis of cervical spine. Echocardiogram was normal. He was discharged under respiratory team follow up and has been referred to orthopaedic clinic for scoliosis.
Figure 1: Chest X-ray showing a large right sided homogeneous opacity and shift of the mediastinum to right side
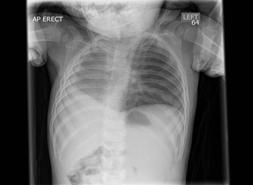
Figure 2: CT thorax showed right pulmonary hypoplasia
Pulmonary hypoplasia is a diagnostic challenge if undiagnosed in antenatal period. It can present in early neonatal period but it is the later infantile and childhood period where we need to keep a high level of suspicion for children with recurrent chest infections and wheeze. (1) Incidence of pulmonary hypoplasia ranges from 9–11 per 10,000 live births and 14 per 10,000 births. (2) Various causes are suggested including genetic factors, viral agents and dietary deficiency of Vitamin A during pregnancy. Secondary hypoplasia is caused by decreased hemithoracic volume, diaphragmatic hernia, decreased pulmonary vascular perfusion, decreased fetal respiratory movement and decreased lung fluid. (3)The clinical presentation depends on degree of pulmonary abnormality and presence of other congenital malformations. Most of the cases present in infancy with recurrent chest infections, cardiopulmonary insufficiency or due to associated congenital anomalies. However many patient may remain asymptomatic. Therefore it can be diagnosed incidentally when complicated by pulmonary infection. Physical examination characteristically reveals asymmetry of two sides. The diagnosis is made based on chest x ray, CT scan and bronchoscopy. (4) CT is the method of choice for the study of congenital lung malformations of thorax, reduction in respiratory movements and absence of air entry in the affected side. The management is conservative in majority of cases and this includes aggressive treatment of chest infections, influenza vaccination and consideration of prophylactic antibiotics in winter months for recurrent chest infections. (5) Surgery is rarely required. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Cadichon SB. Pulmonary hypoplasia. In Kumar P, Burton BK (eds). Congenital malformations: evidence-based evaluation and management. New York: The McGraw-Hill; 2008. p. 143-6.
- Sbokos CG, McMillan IK. Agenesis of the lung. Br J Dis Chest, 1977. 71: 183-97. [CrossRef]
- Page DV, Stocker JT. Anomalies associated with pulmonary hypoplasia. Am Rev Respir Dis. 1982; 125: 216-221. [PubMed]
- Mata JM, Cáceres J, Lucaya J, García-Conesa JA. CT of congenital malformations of the lung. Radiographics. 1990. 10: 651-74. [CrossRef] [PubMed]
- Backer CL, Kelle AM, Mavroudis C, Rigsby CK, Kaushal S, Holinger LD. Tracheal reconstruction in children with unilateral lung agenesis or severe hypoplasia. Ann Thorac Surg. 2009; 88: 624-30. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2016.54
|
| Cite this article as: | | Zafar A, Jeve V. Unilateral Right Pulmonary Hypoplasia with Right Azygous Lobe. Pediatr Oncall J. 2016;13: 110. doi: 10.7199/ped.oncall.2016.54 |
|