Charu Tiwari, Hemanshi Shah, Jyoti Bothra, Vikrant Kumbhar.
Department of Pediatric Surgery, TNMC and BYL Nair Hospital, Mumbai, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Dr Hemanshi Shah, Professor and H.O.D, Department of Pediatric Surgery, TNMC and BYL Nair Hospital, Mumbai 400008, Maharashtra, India.
Email: hemanshisshah@gmail.com | Inflammatory Myofibroblastic Tumor (IMT), first described in adult lungs, is a neoplastic growth of myofibroblasts occurring on a background of plasma cell and lymphocytic proliferation. (1)
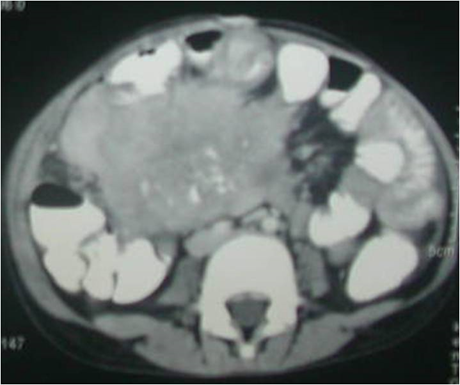
A 7 year-old girl was admitted with lower abdominal lump of six months duration. There was an 8x6cm well-defined firm, smooth, mobile and ovoid lump on the right side of the umbilicus. Chest and abdominal X-rays were normal. Abdominal ultrasound (USG) showed a 10x8x6cm mass in the right side of abdomen, with calcifications and vascularity. Computed Tomography (CT) abdomen revealed an 8.8x7.2x5.4cm ill-defined heterogeneous, enhancing lesion, mostly neoplastic, arising from the mesentery and encasing the small bowel with areas of soft tissue, fat attenuations and calcifications (Figure 1). USG-guided biopsy showed spindle shaped cells on a background of inflammatory infiltrate suggestive of IMT. At laparotomy, a 12x10x8cm firm to hard mesenteric mass, densely adherent to and encasing the ileal loops was found. Complete excision of mass with resection of the adherent bowel and ileo-transverse anastomosis was done. Histopathology revealed that the tumor was composed of interlacing fascicles of elongated spindle cells mixed with plasma cells, histiocytes, lymphocytes and eosinophils, suggestive of IMT. The patient is asymptomatic on follow-up.
Figure 1: Computed Tomography (CT) Scan of the patient showing an 8.8x7.2x5.4cm ill-defined heterogeneous, enhancing lesion, mostly neoplastic, arising from the mesentery and encasing the small bowel; Areas of soft tissue, fat attenuations and calcifications can be seen.
IMT, first described by Brunn in 1939, has been classified as an intermediate neoplasm in the current World Health Organization histologic typing in 2003. (2-4) In children, extra pulmonary IMT occurs in the mesentery, liver, retroperitoneum, bladder, head and neck, extremities, appendix and kidneys. (1) Clinical presentation depends on the site of the tumour. Intra-abdominal tumours present with abdominal lump, distention, fever and weight loss clinically mimicing other intra-abdominal tumours like sarcoma, lymphoma, adenocarcinoma, GIST, desmoid tumor or Carcinoid. (2) Radiological imaging usually reveals a solid well-defined mass with calcifications, often with central necrosis. (1) Percutaneous biopsy is a useful tool for making diagnosis, which depends on the appearance of the myofibroblasts with an inflammatory infiltrate consisting of plasma cells, lymphocytes and occasionally histiocytes. (1,4) Complete surgical resection is the mainstay of cure. (1) Role of chemotherapy, radiotherapy and immunotherapy is minimal and controversial. Diagnosis is histopathological; the differentials being spindle cell tumours of other lineages and pseudo-neoplastic proliferations. Frequent clonal alterations in the chromosome 2p23 have been also found associated. (1) Spontaneous regression by conservative management with antibiotics, steroids or even no treatment have been reported. (4) There has been ambiguity in determining the origin of this tumour-whether it is a post-inflammatory process or a true neoplasm. (1) It is argued that IMT can occur after surgery, trauma, radiotherapy, steroids and also in association with infections like Mycobacterium avium intracellulare, Cornyebacterium, Campylobacter jejuni, Bacillus sphaericus, Coxiella burnetti, Ebstein Barr virus and Escherichia coli. (1,5) The prognosis depends upon the site and age of the patient. (1) Local recurrence and metastasis is common. (1) Long-term follow up with appropriate blood investigations and imaging based on clinical symptoms is mandatory. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Mali VP, Tan HC, Loh D, Prabhakaran K. Inflammatory Pseudotumour of the retroperitoneum- A case report. Ann Acad Med Singapore 2005;34:632-5. [PubMed]
- Chen SS, Liu SI, Mok KT, Whang BW, Yeh MH, Chen YC, et al. Mesenteric inflammatory Myofibroblastic tumours in an elderly with early recurrence: A case report. World J Gastroenterol 2007; 13: 3645-8. [CrossRef] [PubMed] [PMC free article]
- Brunn H. Two interesting benign lung tumours of contradictory histopathology. J Thorac Surg 1939; 9: 119-131.
- Zhao JJ, Ling JQ, Fang Y, Gao XD, Shu P, Shen KT, e al. Abdominal inflammatory Myofibroblastic tumour: Spontaneous regression. World J Gastroenterol 2014; 20(37): 13625-31. [CrossRef] [PubMed] [PMC free article]
- Freud E, Bilik R, Yaniv I, Horev G, Cohen D, Mimouni M, et al. Inflammatory pseudotumour in childhood. A diagnostic and therapeutic dilemma. Arch Surg 1991;126:653-5. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2016.55
|
| Cite this article as: | | Tiwari C, Shah H, Bothra J, Kumbhar V. Pediatric Inflammatory Myofibroblastic Tumor of the mesentery. Pediatr Oncall J. 2016;13: 109. doi: 10.7199/ped.oncall.2016.55 |
|