Minhajuddin Ahmed1, Ashwin A Apte2, Vivek Shukla3, Dipankar Sarkar4, Hari Shankar5.
1Department of Pediatrics, Chirayu Medical College and Hospital, Bhopal, Madhya Pradesh, India,
2Department of Surgery, Peoples Medical College and Hospital, Bhopal, Madhya Pradesh, India,
3Consultant Pathologist, Shagun Pathology, Bhopal, Madhya Pradesh, India,
4Department of Pediatrics, Lake city Hospital, Bhopal, Madhya Pradesh, India,
5Department of Pediatrics, Maxcare Hospital, Bhopal, Madhya Pradesh, India.
ADDRESS FOR CORRESPONDENCE
Dr Minhajuddin Ahmed, Department of Pediatrics, Chirayu Medical College and Hospital, Bhopal, Madhya Pradesh, India.
Email: minzahmad@yahoo.co.in | | Abstract | | Chromobacterium violaceum (CV) is a motile and facultative anaerobic gram-negative bacillus. It is a common inhabitant of soil and water in tropical and subtropical regions. It rarely causes invasive infection in humans and has a high fatality rate. We present a 2 year old boy who presented with ulcerated lesion over right lower chest wall and necrotic skin patch with bacteremia due to CV. He recovered completely with treatment. | | | | Introduction | | Chromobacterium violaceum (CV) is an uncommon human pathogen found mainly in tropical and subtropical weather/climate in contaminated water and soil. (1) Human infection from this pathogen is extremely rare and has a very high mortality rate. (2) Clinical manifestations of CV include rapidly progressive sepsis, visceral abscesses, skin and soft tissue infection mainly in lungs, liver and spleen. (3, 4) Till now around 150 cases has been reported in literature and nine cases have been reported from India. (5) We present a case a 2 year old boy who presented with ulcerated lesion over right lower chest wall and necrotic skin patch with septicemia due to CV. He recovered completely with treatment. | | | | Keywords | | Chromobacterium violaceum, septicemia | | | | Case Report | A 2 years old boy was referred to our hospital with fever for 7 days and a small papule on right side of chest that evolved into an abscess followed by ulceration. On admission, patient was febrile, had pallor, was toxic looking with heart rate of 115 beats/min, respiratory rate of 28/min, blood pressure of 84/55 mm of mercury (Hg). There was an ulcerated lesion over right lower chest wall and necrotic skin patch with surrounding erythema and induration. He also had a small subcutaneous nodule over right lower leg and left side of the back over the scapula. Systemic examination was normal. Laboratory investigations showed hemoglobin 8.9 gm/dL, total leucocyte count 29,800/cumm (neutrophils 68%, lymphocyte 22%, eosinophils 4%), platelet count 266,000/cumm, ESR 60 mm/ at end of 1 hour, C- reactive protein 116 mg/dL. Renal and liver function tests were normal. Chest radiograph was normal. Swab and pus culture from the chest wall wound did not grow any organism. Blood culture grew chromobacterium violaceum (Figure 1). On subsequent inquiry, it was found that the child had gone for a picnic where he had taken bath in a waterfall, ten days prior to fever. He was treated with intravenous ceftriaxone and amikacin initially with no improvement, later it was upgraded to meropenem which led to improvement. He received meropenem for 21 days. Workup for immunodeficiency could not be done in our patient.
Figure 1: Blood culture showed colonies of chromobacterium violaceum as pigmented strains giving a violet pigment known as violacen
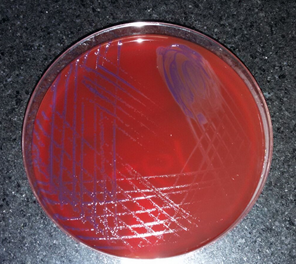
| | | | Discussion | | CV is a motile gram-negative, catalase-positive, non-spore forming, facultative anaerobic, rod-shaped bacterium. CV is an inhabitant of soil and water which usually grows on blood agar, Mac Conkey’s agar and Mueller-Hinton. CV gives pigmented and non-pigmented strain but non-pigmented strains are rare. Pigmented strains give a violet non-diffusible pigment known as violacen. (6) Clinical manifestation includes skin and soft tissue, liver, lung and splenic abscesses. Other manifestations include pneumonia, diarrhea, urinary tract infection, conjunctivitis, purulent otitis externa with mastoiditis, meningitis and osteomyelitis. (7-9) Route of entry of this pathogen is unclear but is usually seen in traumatic/wounded skin lesion or oral. (10) Our patient did not have any history of trauma but had taken a bath in a waterfall. However port of entry is unclear in our patient. Predisposition to CV infection is seen in patients of chronic granulomatous disease and those with Glucose-6-Phosphate Deficiency as neutrophils are unable to produce reactive oxygen species/ metabolites required to kill the phagocytosed bacteria. (11) This inadequacy makes the patients vulnerable to frequent infections which may spread unabated lead to septicemia. Certain strains of CV have the ability to produce an endotoxin which makes them resistant to phagocytosis. Rate of mortality in children is about 40-50% while risk for mortality is young age, localized abscess, short clinical course and inappropriate treatment. (12) CV is usually resistant to penicillin and narrow spectrum cephalosporins while response to third generation cephalosporin is variable. Broad spectrum cephalosporins, carbapenems and fluoroquinolones are advised though the recommended antimicrobial therapy for CV is not established or clear. | | | | Conclusion | | High suspicion for CV infection should be considered in a patient who does not show improvement with routine antibiotics. Because of its rarity and high mortality rate, appropriate therapy should be administered timely to reduce mortality. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- von Graevenitz A, Zbinden R, Mutters R. Actinobacillus, capnocytophaga, Eikenella, Kingella, and other fastidious or rarely encountered gram-negative rods. In: Murray PR, Baron EJ, Pfaller MA, Tenover F, Yolken RH, eds. Manual of clinical microbiology. 8th ed. Washington, DC: American Society of Microbiology Press; 2003:603-20.
- Steinberg JP, Del Rio C. Other gram-negative and gram-variable bacilli. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and practice of infectious diseases. 6th ed. Philadelphia: Churchill Livingstone; 2005:2751-68.
- Sneath PH, Whelan JP, Bhagwan Singh R, Edwards D. Fatal infection by Chromobacterium violaceum. Lancet. 1953;265:276-7. [CrossRef]
- Shao PL, Hsueh PR, Chang YC, Lu CY, Lee PY, Lee CY, Huang LM. Chromobacterium violaceum infection in children: a case of fatal septicemia with nasopharyngeal abscess and literature review. Pediatr Infect Dis J. 2002 Jul;21(7):707-9. [CrossRef] [PubMed]
- Ray P, Sharma J, Marak RS, Singhi S, Taneja N, Garg RK, Sharma M. Chromobacterium violaceum septicemia from North India. Indian J Med Res, 2004; 120:523-526. [PubMed]
- James I, Campbell A. Successful antimicrobial regime for Chromobacterium violaceum induced Bacteraemia. BMC Infect Dis. 2013. 13:4. [CrossRef] [PMC free article]
- Lee TS, Wright BD. Fulminating chromobacterial septicemia presenting as respiratory distress syndrome. Thorax. 1981; 36: 557-559. [CrossRef]
- Jitmuang A. Human Chromobacterium violaceum infection in South-East Asia. South Asian J Trop Med Public Health. 2008;39:452–460. [PubMed]
- Shetty M, Venkatesh A, Shenoy S, Shivananda PG. Chromobacterium violaceum meningitis: a case report. Ind J Med Sci 1987; 41: 275-276.
- Grier DD, Qiu J, Rand K, Donnelly WH. Pathologic quiz case: a 13 year- old boy with a 2-day history of fever, vomiting and mental status changes. Chromobacterium violaceum bacteraemia. 2004;128: e131-132.
- Ponte R, Jenkins SG. Fatal Chromobacterium violaceum infection associated with exposure to stagnant water. Pediatr Infect Dis J. 1992;11: 583-586. [CrossRef]
- Sirinavin S, Techasaensiri C, Benjaponpitak S, Pornkul R, Vorachi M. Invasive Chromobacterium violaceum infection in children: case report and review. Pediatr Infect Dis J. 2005;24:559-61. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2017.17
|
| Cite this article as: | | Ahmed M, Apte A A, Shukla V, Sarkar D, Shankar H. Chromobacterium Violaceum Bacteremia in a 2 Years old Male Child. Pediatr Oncall J. 2017;14: 43-44. doi: 10.7199/ped.oncall.2017.17 |
|