Rahul Sinha, Vinod Sharma, Raghav Sharma, Kavita Pandey.
Department of Pediatrics, Military Hospital, Jodhpur, India.
ADDRESS FOR CORRESPONDENCE
Lt Col (Dr) Rahul Sinha, HOD Pediatrics, Military Hospital, Jodhpur, India.
Email: drrahul_2000@yahoo.com | | Abstract | | Bone is a complex organ that is metabolically active, particularly in children. Normal metabolism is dependent upon the three main elements: matrix, mineral and cells that are integral components of bone. In addition there are several hormonal factors that also influence bone metabolism. Abnormalities in any of these components can give rise to metabolic bone disease. The manifestations of deficiency may vary from hypocalcemic seizures, tetany in infancy and adolescence to florid rickets in toddlers. Treatment is necessary for all individuals with deficiency whether symptomatic or not and consists of vitamin D supplementation as Stoss therapy or daily or weekly oral regimens with equal efficacy and safety, combined with calcium supplements. In this article we present three different cases of metabolic bone disease with varied features which the clinician should keep in mind while dealing with these cases. This case series adds a wide spectrum to the diagnosis and management of metabolic bone disease. | | | | Keywords | | rickets, fracture, vitamin D, Calcium | | | | Introduction | Bone is a complex organ that is metabolically active, particularly in children. Normal metabolism is dependent upon the three main elements: matrix, mineral and cells that are integral components of bone. In addition there are several hormonal factors that also influence bone metabolism. Abnormalities in any of these components can give rise to metabolic bone disease. Abnormalities of mineralization are the commonest manifestation of metabolic bone disease although some are ultimately derived from problems within the supporting cellular components. Vitamin D deficiency is considered to be the most common nutritional deficiency (1) and also one of the most common undiagnosed medical conditions in the world. Vitamin D has evolved into a hormone that is active throughout the body not only to regulate calcium and bone metabolism but also to reduce the risk of chronic diseases including auto immune diseases, malignancies, cardiovascular and infectious diseases. It has been estimated that 1 billion people worldwide have vitamin D deficiency or insufficiency. (2) Though majority of population in India lives in areas receiving ample sunlight throughout the year, vitamin D deficiency is very common in all the age groups and both the sexes across the country. (3) Vitamin D deficiency is defined as serum levels of 25(OH) D less than 20 ng/d whereas 21- 29 ng/dL is considered to be insufficient by US Endocrine Society. (2,3) We present 3 different cases of metabolic bone disease in different age group.
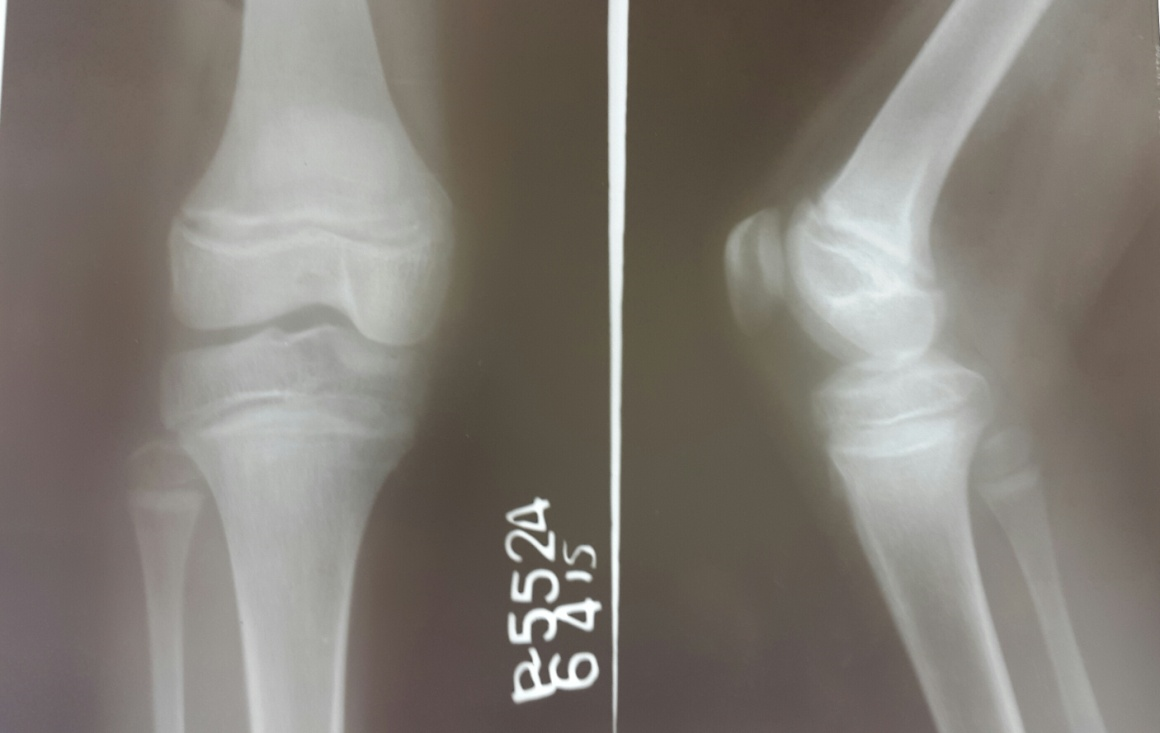
Case 1: An 11 years old girl born of non-consanguineous marriage presented with 3-4 episodes of carpopedal spasms in last 14 days. The dietary (2500kcal/28gms of protein) intake was adequate. Clinical examination revealed height of 140cm (10-25 percentile), weight of 31kgs (10-25 percentile). General and systemic examination was normal. Chovstek sign (fig 1) was positive with carpopedal spasm involving hand and feet. Investigations showed normal hemogram, urine examination and thyroid function tests. Other metabolic work-up is depicted in table 1. Electrocardiogram (ECG) showed long QTc of 0.47sec (fig 2). X-ray Knee joint shows haziness and irregularity at metaphyseal end (Fig 3). Chest X-ray was normal. She was thus diagnosed as hypocalcemic tetany with Vitamin D deficiency. She was started on IV calcium gluconate (5ml in 10ml normal saline slowly over 30 min under cardiac monitor). Subsequently she was treated with vitamin D supplements of cholecalciferol (60000U weekly for 4weeks then monthly for 3 months) along with calcium and phosphate supplements. She was asked to follow up regularly.
Fig 1: Carpopedal spasm

Fig 2: ECG showing long QTc 0.47 sec

Fig 3: X-rays of the knee showing haziness and irregularity at metaphyseal end
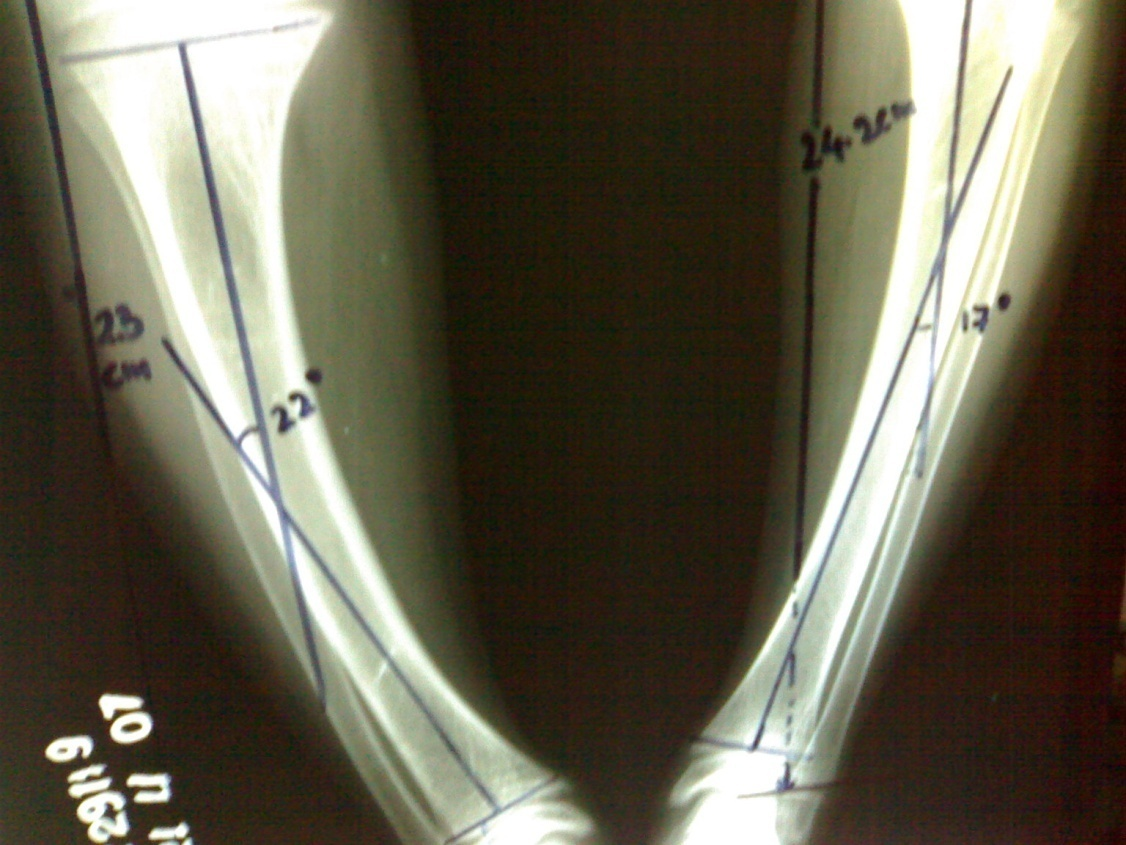
Case 2: A 10 years old female child born of non-consanguineous marriage presented with progressive bowing of legs since 3 years of age associated with polyuria and polydipsia. She was not gaining weight. She took a daily diet of 2000 Kcal and 20 gms of protein. On examination, height was 108 cm (<5th percentile), weight was 21kgs (<5th percentile) with upper segment: lower segment ratio of 1.07:1. Father’s height was 170 cm and mother’s height was 158 cm. Mid-parental height was: 157.5 cm + 6.5 cm. She had bowing of legs (Fig 4). X-ray femur and tibia revealed femur bowing bilaterally 30o and tibia bowing (right 220, left 17o.) (Fig 5). There were no other bony deformities. Investigations showed normal hemogram, urine examination and thyroid function tests. Other metabolic work –up is depicted in table 1. Bone age was 8-11years. Tubular reabsorption of phosphate (TRP) was 67% (Normal >90%). She was diagnosed as hypophosphatemic rickets and started on Joulie’s solution (Monosodium diphosphate with disodium monophosphate) in a dose of 10ml every 4hourly along with vitamin D supplements of cholecalciferol 60000U weekly for 4weeks then monthly along with calcium supplements. We wanted to achieve a 25 hydroxy vitamin D3 level of around 70 nmol/L, hence vitamin D supplements were given. Orthopedic consultation was taken and she was planned for corrective osteotomy.
Fig 4: Bowing of legs

Fig 5a: X-rays of lower limbs showing femur bowing bilaterally 30 Degree

Fig 5b: X-rays of lower limbs showing tibia bowing (right 22 Degree, left 17 Degree)
Case 3: A 23 months old girl presented with swelling and pain in right thigh following a fall from a chair. Dietary history revealed intake of 1200 Kcal and 14 gms of protein. On examination, weight was 12 kg (10-25th percentile), height was 87cm (25-50th percentile). There was swelling and tenderness at middle third of right thigh. She had wrist widening. Other systems were normal. Investigations showed normal hemogram, urine examination and thyroid function tests. Other metabolic work –up is depicted in table 1. X-ray femur revealed transverse fracture of shaft of right femur (Fig 6) and X-ray wrist revealed fraying and splaying of the metaphyseal ends of both the radius and ulna with widening of metaphyses (Fig 7). She was diagnosed to have nutritional rickets. She was given Inj Vit D 600,000 units which was repeated after 3 weeks and gallows traction was applied. Repeat x ray of the wrist revealed healing line at metaphysical end after 3 weeks (Fig 8).
Fig 6: X-ray showing fracture of right femur in middle third

Fig 7: X-ray of the wrist showing fraying and splaying of the metaphyseal ends of both the radius and ulna with widening of metaphyses

Fig 8: X-ray of the wrist showing healing line at metaphysical end after 3 weeks

Table 1: Metabolic workup of all the patients
| |
Patient 1 |
Patient 2 |
Patient 3 |
| Serum calcium (mg %) (Normal: 9-11 mg %) |
7.9 |
|
|
| Ionic calcium (mg %) (Normal: 4-5 mg %) |
2.6 |
4 |
3.2 |
| Phosphorus (mg/dl) (Normal: 2.5-4.5mg/dl) |
3.9 |
2 |
3.9 |
| Alkaline phosphatase (IU/L) (Normal: 400-800 IU/L) |
778 |
778 |
900 |
| Magnesium (mg/dl) (Normal: 1.70-2.10 mg/dl) |
1.80 |
- |
- |
| Serum albumin (gm/dl) |
3.8 |
- |
- |
| 24 hours urine calcium (mg) (Normal: 100-300) |
250 |
280 |
- |
| 24 hours urine phosphorus (mg) (Normal: 400-800) |
500 |
820 |
- |
| Serum parathyroid hormone (PTH) (pg/dl) (Normal: 10-69 pg/dl)) |
605 |
22.9 |
- |
| 25 hydroxy cholecalciferol (nmol/l) |
<10 |
54.38 |
- |
| 1,25 dihydroxy cholecalciferol (pmol/l) (Normal: 39-193 pmol/l)) |
15.32 |
37.32 |
- |
| pH |
7.4 |
7.38 |
- |
| Bicarbonate (meq/L) |
22 |
21 |
- |
| Serum sodium (meq/L) |
140 |
140 |
140 |
| Serum potassium (meq/L) |
4.5 |
4.5 |
4.5 |
| Serum chloride (meq/L) |
110 |
110 |
110 |
| Blood urea nitrogen (BUN) (mg %) |
19 |
13 |
13 |
| Serum creatinine (mg %) |
0.9 |
0.6 |
0.6 |
| | | | Discussion | Metabolic bone disease in children includes many hereditary and acquired conditions of diverse etiology that lead to disturbed metabolism of the bone tissue. Some of these processes primarily affect bone; others are secondary to nutritional deficiencies, a variety of chronic disorders, and/or treatment with some drugs. Some of these disorders are rare, but some present public health concerns (for instance, rickets) that have been well known for many years but still persist. (4-6) The most important clinical consequences of bone metabolic diseases in the pediatric population include reduced linear growth, bone deformations, and non-traumatic fractures leading to bone pain, deterioration of motor development and disability.
Rickets is the most common metabolic bone disease in the world and is easily treatable as well as preventable with sun exposure and dietary supplementation. (4) Infants and adolescents are predisposed to rickets secondary to increased flux in body composition and rates of rapid bone growth causing increased need/utilization of calcium and phosphate. Further increased risk is associated with dark-skinned individuals, lack of UV-B exposure, solely breastfed infants and prematurity. Screening should be considered for children with poor growth/development, seizure activity/tetany, and children with chronic malabsorptive states. It is estimated that worldwide there are around 1 billion cases of vitamin D deficiency and around 80% of healthy Indian are vitamin D deficient as per diabetes foundation of India (3). This deficiency is observed among breast fed babies at one end and with dietary calcium deficiency in older children at the other end.
In this article we presented three different cases of metabolic bone disease with varied features which the clinician should keep in mind while dealing with similar cases. The management of metabolic bone disease depends on the types of rickets and associated deficiency. The treatment for rickets may be administered gradually over several months or in a single-day dose of 15,000 mcg (600,000 U) of vitamin D. Also daily dose of 125-250 mcg (5000-10,000 U) can be given for 2-3 months until healing is well established and the alkaline phosphatase concentration is approaching the reference range. Because this method requires daily treatment, success depends on compliance. If the vitamin D dose is administered in a single day, it is usually divided into 4 or 6 oral doses. An intramuscular injection is also available. Vitamin D (cholecalciferol) is well stored in the body and is gradually released over many weeks. The supplement with calcium should continue for at least 3-4 month. The treatment of hypophosphatemic rickets is done by administration of phosphate solution (Joulie’s solution). This case series adds a wide spectrum to the diagnosis and management of metabolic bone disease. So early identification and treatment of potential risk factors is essential for skeletal health in adulthood. In most conditions it is necessary to ensure an appropriate diet, with calcium and vitamin D, and an adequate amount of physical activity as a means of prevention (8). | | | | Conclusion | | This case series adds a wide spectrum to the diagnosis and management of metabolic bone disease. Education on proper nutrition during pregnancy and supplementation during breastfeeding is necessary to prevent its growing resurgence. Proper childhood maintenance visits with growth and development screenings are critical for early detection of this easily treatable condition. | | | | Contributor Statement | | All authors contributed towards manuscript layout. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Holick MF. Vitamin D: extraskeletal health. Rheum Dis Clin North Am. 2012; 38:141-60. [CrossRef]
- Harinarayanan CV, Joshi SR. Vitamin D status in India – Its implications and remedial measures. J Assoc Physicians. 2009;57: 40-8.
- Marwaha RK, Sripathy G. Vitamin D and Bone mineral density of healthy school children in northern India. Indian J Med Res. 2008;127:239-44. [PubMed]
- Dimitri P, Bishop N, Rickets: New insights into a re-emerging problem. Curr Op in Ortho. 2007; 18: 486-493. [CrossRef]
- Chapman T, Sugar N, Done S, Marasigan J, Wambold N, Feldman K. Fractures in infants and toddlers with rickets. Pediatr Radiol. 2010 Jul;40(7):1184-9. [CrossRef]
- Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M; Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D deficiency in children and its management. Review of current knowledge and Recommendations. Pediatrics. 2008;122;398. [CrossRef]
- Litonjua AA. Childhood asthma may be a consequence of vitamin D deficiency. Curr Opin Allergy Clin Immunol.2009;9: 202-7. [CrossRef] [PMC free article]
- Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children and adolescents. Pediatrics. 2008;122:1142-52. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2017.47
|
| Cite this article as: | | Sinha R, Sharma V, Sharma R, Pandey K. SPECTRUM OF METABOLIC BONE DISEASE - A CASE SERIES. Pediatr Oncall J. 2017;14: 35-38. doi: 10.7199/ped.oncall.2017.47 |
|