|
Chest Pain in the Emergency Department
Benedita Bianchi de Aguiar, Tatiana Pereira, Alexandra Martins, Magalys Pereira, Miguel Costa.
Department of Pediatrics, Centro Hospitalar Entre Douro e Vouga, Porto, Portugal.
ADDRESS FOR CORRESPONDENCE
Benedita Bianchi de Aguiar, Rua Marta Mesquita da Câmara 175 hab 62 4150-282, Porto, Portugal.
Email: beneditabaguiar@gmail.com
Due to the physical examination as well as the medical history presented she underwent a chest x-ray and CT chest.
Figure 1. Chest X-ray

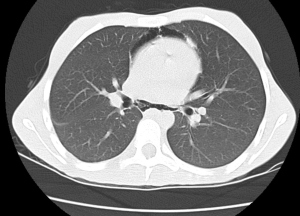
Figure 2. CT chest
|
Figure 1. Chest X-ray

|
What is the diagnosis?
Chest x-ray showed hypotransparency of the paracardiac mediastinum with a discrete air lamina involving the cardiac silhouette. Computed tomography scan revealed a pneumomediastinum affecting all compartments and extending to the cervical region with coexisting emphysema of the superior thoracic wall.
Pneumomediastinum results from the dissociation of the air of the pulmonary parenchyma within the mediastinum. It is commonly a self-limited process, without the need for aggressive intervention and occurs mainly in male adolescents. The most frequent symptom is chest pain – which our adolescent reported.1 The most common causes are asthma exacerbations, bronchospasm, cough, respiratory tract infection, and vomiting. These are activities that require the Valsalva maneuver.2 On further enquiry in our patient, it was found that the adolescent had been taught some respiratory exercises, which she did daily at home. After being questioned she recalled her symptoms has begun the day before after she had done her respiratory exercises due to severe school-related anxiety.
The diagnosis is confirmed by a chest x-ray, although it may be helpful to perform a CT-scan in order to better characterize the clinical condition as well as detect possible complications.3 The treatment is conservative and essentially symptomatic1; however, it is necessary to exclude and underlying pulmonary conditions. Prognosis is favorable in most cases. |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Chen I-C, Tseng C-M, Hsu J-H, Wu J-R, Dai Z-K. Spontaneous pneumomediastinum in adolescents and children. Kaohsiung J Med Sci. 2010;26:84–8. [CrossRef]
- Gasser CR-B, Pellaton R, Rochat CP. Pediatric Spontaneous Pneumomediastinum: Narrative Literature Review. Pediatr Emerg Care. 2017;33:370–4. [CrossRef] [PubMed]
- Kouritas VK, Papagiannopoulos K, Lazaridis G, Baka S, Mpoukovinas I, Karavasilis V, et al. Pneumomediastinum. J Thorac Dis. 2015;7(Suppl 1):S44-9. [PubMed] [PMC free article]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2019.6 |
| |
Cite this article as:
Aguiar B B d, Pereira T, Martins A, Pereira M, Costa M. Chest Pain in the Emergency Department. Pediatr Oncall J. 2019;16: 28. doi: 10.7199/ped.oncall.2019.6
|