Satheeshkumar D, Kumaravel K S, Karuna C, Hemalatha M, Sampathkumar P.
Government Mohan Kumaramangalam Medical College Hospital, Salem, Tamilnadu, India.
ADDRESS FOR CORRESPONDENCE
Dr Kumaravel K S, 191A, Shankar Nagar, Salem 636007, Tamilnadu, India.
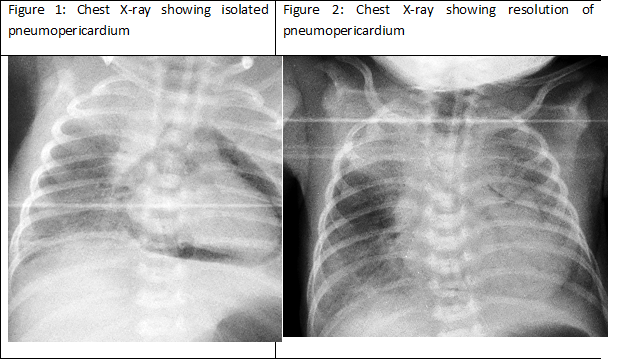
Email: kumaravelks@rediffmail.com | A preterm 34 week male, weighing 2 kg was admitted with respiratory distress at birth. He was started on Continuous Positive Airway Pressure (CPAP) ventilation and early rescue surfactant was administered. At 6 hours of life, the respiratory distress worsened. Chest X- ray revealed isolated pneumopericardium (PPC) with bilateral upper lobe pneumonia (Figure 1). Echocardiogram confirmed the PPC and there were no evidence of tamponade. Since the baby was hemodynamically stable, a conservative approach was followed with invasive ventilation with higher oxygen concentration. Repeat chest X-ray (Figure 2) and echocardiogram after 24 hours of life showed resolution of PPC and appearance of a minimal pneumothorax on the right side which was also managed conservatively. The neonate died on the third day of life due to worsening respiratory distress syndrome (RDS).
Air leak syndromes are common in neonates with hyaline membrane disease due to over distension of premature alveoli. (1) Other predisposing factors contributing to air leak are active mechanical ventilation, CPAP and meconium aspiration. Neonatal PPC is one such rare complication which can occur in isolation or in association with pneumomediastinum, pulmonary interstitial emphysema and pneumothorax. But isolated PPC is a much rarer event which has a high morbidity and mortality. Though its mechanism is poorly understood one common theory involves leakage of air from the ruptured alveoli and entering into the perivisceral fascia of the hilum and into the pericardial space. (2) This trapped air decreases the venous return to the heart and compresses the pulmonary veins resulting in circulatory collapse. Clinical features vary from asymptomatic presentation to a range of clinical features that signifies cardiac tamponade including tachycardia, bradycardia, hypotension, cyanosis, muffled heart sounds and shock. (3) It is imperative to diagnose PPC and differentiate it from other air leak syndromes, especially pneumomediastinum as these may have clinical features and radiological appearances that are difficult to differentiate. The signs of PPC include 1) halo sign which is a band of air around the cardiac silhouette which doesn’t extend beyond the greater vessels, 2) presence of infra cardiac air shadow, 3) concavity of pericardium is placed medially whereas in pneumomediastinum it is towards the periphery, 4) lateral X- ray shows air around the heart in contrast to pneumomediastinum where air shadow is seen behind the sternum only. (4)
Treatment of PPC is confusing and challenging till date and the decision for invasive procedures depends on presence of overt clinical signs of cardiac tamponade. In asymptomatic cases, a conservative approach and supportive care is the cornerstone. Hundred percent oxygen therapy which causes nitrogen washout can be used in stable infants but not in premature babies less than 32 weeks due to complications of hyperoxia. (5) Percutaneous pericardial aspiration can be attempted in case of hemodynamic instability due to tamponade. Continuous pericardial drainage can be used in recurrent and extensive cases.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Junghaenel S, Sreeram N, Demant A, Vierzig A, Kribs A, Roth B. Pneumopericardium as a rare complication of continuous positive airway pressure in spontaneously breathing neonates. Klin Paediatr. 2012; 224: 34–5. [CrossRef] [PubMed]
- Varano LA, Maisels MJ. Pneumopericardium in the newborn: diagnosis and pathogenesis. Pediatrics. 1974; 53: 941–945. [PubMed]
- Roychoudhury S, Kaur S, Soraisham AS. Neonatal Pneumopericardium in a Non-ventilated Term Infant: A Case Report and Review of the Literature. Case Rep Pediatr. 2017;2017: 3149370.
- Burt TB, Lester PD. Neonatal pneumopericardium. Radiology. 1982; 142: 81–84. [CrossRef] [PubMed]
- Suresh P, Tagare A, Kadam S, Vaidya U, Pandit A. Spontaneous pneumopericardium in a healthy full-term neonate. Indian J Pediatr. 2011;78:1410-1411. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2018.41
|
| Cite this article as: | | D S, S K K, C K, M H, P S. A Case of Conservatively Managed Pneumopericardium in a Neonate. Pediatr Oncall J. 2018;15: 114. doi: 10.7199/ped.oncall.2018.41 |
|