Parminder Singh1, Divya Gupta2.
1Department of Pediatrics, Base Hospital, Tezpur, Assam, India,
2Department of Pathology, Base Hospital, Tezpur, Assam, India.
ADDRESS FOR CORRESPONDENCE
Parminder Singh, MD Pediatrics, 155 Base Hospital, Tezpur, Assam-784001.
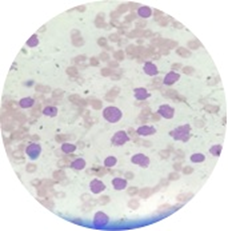
Email: param_rules@yahoo.co.in | A one and half month old male infant born at term was brought with progressive abdominal distension since 1 month of age along with reduced acceptance of feeds with increased chest activity. Baby was born to 23 years old primigravida by normal vaginal delivery and had a birth weight of 2.75 kg. On examination, he was pale, febrile and tachypneic. There was no dysmorphism. He had respiratory distress with subcostal, intercostal recession along with wheeze and crepitations with massive spleen and liver enlargement. External genitalia were normal. Initial hematological investigations revealed a hemoglobin level of 8.4 gm/dl, total leukocyte count of 170,000/cumm and platelet count of 49,000/cumm. Peripheral blood smear showed numerous atypical cells which were large in size with high nuclear: cytoplasmic ratio, open chromatin with multiple nucleoli (Figure 1). Serum electrolytes revealed mild hyponatremia (131meq/dl) and hyperkalemia (potassium: 6.1meq/dl). Serum LDH (1020 IU/l) and uric acid (12.3 mg/dl) levels were markedly raised. Chest x-ray revealed extensive infiltrates bilaterally which were suggestive of bronchopneumonia, more in the upper zone. TORCH IgM were negative and blood culture was sterile. Bone marrow aspiration revealed blasts expressing myeloid markers (CD13, CD33, CD14, CD117, HLA DR) positivity with absence of lymphoid markers. A diagnosis of acute myeloid leukemia (AML) French‐American‐British (FAB) type M5, was made. Cytogenetic investigation revealed a normal 46XY karyotype. Unfortunately before the induction of chemotherapy baby expired due to multiple complications. Testing for MLL gene rearrangement and post mortem could not be due the unwillingness of the parents.
Figure 1. Peripheral smear showing atypical cells which are large in size, high nuclear: cytoplasmic ratio, open chromatin and prominent nucleoli
The incidence of congenital leukemia is 1 in half a million live births and represents < 1% of all childhood leukemia. The congenital leukemia comprise of mostly AML and lesser extent of acute lymphocytic leukemia (ALL) unlike older children where ALL seen to be predominant.(1,2,3) Many risk factors such as maternal exposure to occupational, environmental toxins and radiation have been implicated. (2) Clinical presentation ranges from hepatosplenomegaly, petechiae, ecchymosis to non-specific symptoms. Many infants develop severe respiratory distress due to either leukemic infiltrates with atelectasis or secondary to bronchopneumonia. In our patient, we could not determine whether the child had leukemic infiltrates in the lung or had bronchopneumonia as the child died before we could investigate further. Leukemia cutis is commonly found when the disease appears at birth. (1) Diagnosis of congenital leukemia involves assessing the cellular morphology, cytochemistry, flow cytometry and chromosomal studies. It is important to differentiate congenital leukemia from conditions such as bacterial infections, hypoxemia and severe hemolysis in the neonates. (1-4) Most important differential diagnosis is transient myeloproliferative disease (TMD) associated with Down’s syndrome. FAB classification based on cell morphology reveals that the most common subtype in infantile and neonatal acute non-lymphocytic leukemia is the monocytic variety which was also the case in our patient. (1,2) Over the years, management of congenital leukemias has seen a paradigm change. However despite aggressive chemotherapy the outcome continues to be poor in most cases (5). Hence this warrants further research into the possible etiological factors and newer management protocols to improve the mortality rates.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Bresters D, Reus AC, Veerman AJ, van Wering ER, van der Does-van den Berg A, Kaspers GJ. Congenital leukaemia: the Dutch experience and review of the literature. Br J Haematol. 2002;117:513-24. [CrossRef] [PubMed]
- Tewari VV, Mehta R, Tewari K. Congenital Acute Leukemia: A Rare Hematological Malignancy. J Neonatal Biol 2017; 6: 265. DOI: 10.4172/2167-0897.1000265 [CrossRef]
- Sethi RS, Sethi A. Congenital leukemia. Indian Pediatr. 2002; 39:497-500. [PubMed]
- Raghavendra P, Naveen K. Congenital leukemia in a 2-month old boy. The Internet Journal of Pediatrics and Neonatology. 2006;6:2. Available at URL: http://ispub.com/IJPN/6/2/10690. Accessed on 5th Nov 2018.
- Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med. 2006;354:166-78. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2018.42
|
| Cite this article as: | | Singh P, Gupta D. Respiratory Distress without Heart Failure - A Presentation of Congenital Leukemia. Pediatr Oncall J. 2018;15: 112-113. doi: 10.7199/ped.oncall.2018.42 |
|