|
Right Sided Cerebellar Ataxia with Occipital Encephalocele (Arnold -Chiari Type III Malformation)
Parminder Kaur, Jaswir Singh, Manpreet Kaur.
Department of Pediatrics, GMC Patiala, Punjab, India.
ADDRESS FOR CORRESPONDENCE
Dr Parminder Kaur, House No 3079, Rajpura town, District Patiala, Punjab, India
Email: kaurparminder1991@yahoo.in
Chiari malformation, chiari III, posterior encephalocele
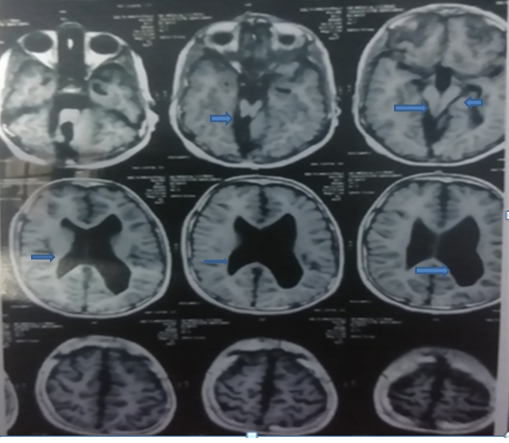
A 7 years old male child with global developmental delay presented with recurrent falls on the right side while walking for 15 days. He had 2 episodes of generalized tonic-clonic seizures 2 years ago for which he was taking sodium valproate at a dose of 20 mg/kg/day following which he was seizure-free. He also had occipital encephalocele at birth for which he was operated on day 2 of life. On examination, signs of cerebellar ataxia were present with ataxia involving the right side predominantly. Other systems were normal. MRI brain revealed supratentorial ventricular dilation, the parallelism of walls of 3rd ventricle with a diameter of 9.5 mm, grey matter heterotopias in the frontal lobe, distorted elongated 4th ventricle communicating with fluid spaces in post fossa on the right side and non-visualization of the right-sided cerebellar hemisphere (Figure 1).
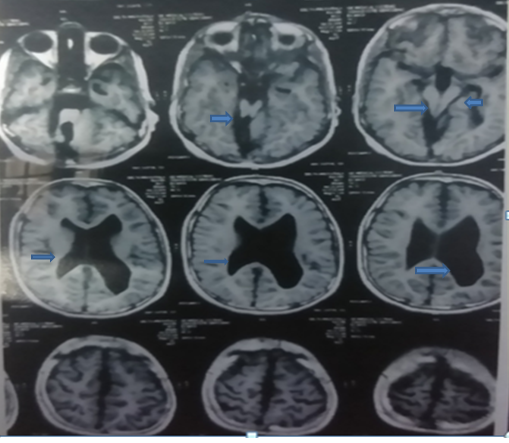
Figure 1. MRI brain showing supratentorial ventricular dilation with distorted elongated 4th ventricle communicating with fluid spaces in post fossa on right side and non-visualization of the right sided cerebellar hemisphere with parallelism of walls of 3rd ventricle
|
Figure 1. MRI brain showing supratentorial ventricular dilation with distorted elongated 4th ventricle communicating with fluid spaces in post fossa on right side and non-visualization of the right sided cerebellar hemisphere with parallelism of walls of 3rd ventricle
|
What is the diagnosis?
Arnold Chiari malformation type III. Chiari malformations involve the hindbrain and cervical spinal cord. There are four types of Chiari malformation: (i) Chiari I: there is more than 5-mm descent of the caudal tip of cerebellar tonsils past the foramen magnum, (ii) Chiari II: Brainstem, fourth ventricle, and more than 5-mm descent of the caudal tip of cerebellar tonsils past the foramen magnum associated with spina bifida, (iii) Chiari III: involves herniation of the cerebellum with or without the brainstem through a posterior encephalocele and (iv) Chiari IV: there is cerebellar hypoplasia or aplasia with normal posterior fossa and no hindbrain herniation.1 Type III is a rare type of Chiari malformation and the most severe one. Arnold Chiari malformation type III is associated with occipital encephalocele (containing neuroectodermal tissue), hydrocephalus, tethered cord, elongation of the fourth ventricle, failure of development of pontine flexure and kinking of the brainstem, pons, inferior vermis.2 Occipital bone defects are seen in some, but not all Chiari III malformations,3 and 70% of cases have been reported to have an incomplete fusion of the posterior arches of C1.2 Contents of encephalocele in Chiari malformation III is usually non-functional and contains necrosis of neural tissue, gliosis, fibrosis, meningeal inflammation, cerebral or cerebellar tissue, ventricles, and reactive astrocytes.4,5 Clinical findings may range from asymptomatic incidental finding to severe neurological deficit being gait spasticity, in-coordination, otoneurologic symptoms (dizziness, hearing loss, vertigo), and recurrent headaches.1 The treatment of choice is surgical decompression of posterior fossa in form of craniectomy or spinal laminectomy. Hydrocephalus can be relieved by shunting. Early the surgery, better is the prognosis.1 |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Hidalgo JA, Varacallo M. Arnold Chiari Malformation. [Updated 2018 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431076/. Accessed on 31st August 2019
- Cakirer S. Chiari III malformation: varieties of MRI appearances in two patients. Clin Imaging. 2003; 27:1-4. [CrossRef]
- Aribal ME, Gürcan F, Aslan B. Chiari III malformation: MRI. Neuroradiology. 1996 May;38 Suppl 1: S184-6. [CrossRef] [PubMed]
- Işik N, Elmaci I, Silav G, Celik M, Kalelioğlu M. Chiari malformation type III and results of surgery: a clinical study: report of eight surgically treated cases and review of the literature. Pediatr Neurosurg. 2009; 45:19- 28. [CrossRef] [PubMed]
- Castillo M, Quencer RM, Dominguez R. Chiari III malformation: imaging features. AJNR Am J Neuroradiol. 1992; 13(1): 107-113.
|
|
DOI: https://doi.org/10.7199/ped.oncall.2020.15 |
| |
Cite this article as:
Kaur P, Singh J, Kaur M. Right Sided Cerebellar Ataxia with Occipital Encephalocele (Arnold -Chiari Type III Malformation). Pediatr Oncall J. 2020;17: 64-65. doi: 10.7199/ped.oncall.2020.15
|