|
Rigler's Sign
Catarina Santiago Gonçalves1, Dora Fontes2, Vasco Herédia3, Maria José Mendes2.
1Pediatric Services, Department of Women's and Children's Health, Espírito Santo Hospital of Évora, Évora, Portugal,
2Neonatology Unit, Department of Women's and Children's Health, Espírito Santo Hospital of Évora, Évora, Portugal,
3Imaging Service, Espírito Santo Hospital of Évora, Évora, Portugal.
ADDRESS FOR CORRESPONDENCE
Catarina Santiago Goncalves, Largo do Sr. da Pobreza, 7000-811 Evora, Portugal.
Email: catarina.sg@hotmail.com
Rigler's sign, pneumoperitoneum, radiograph
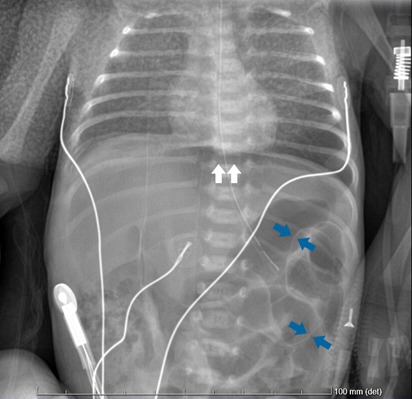
A male infant born at 31 weeks and 6 days of gestation by vaginal delivery with a birth weight of 1785 g had Apgar score of 8 and 9 at 1 and 5 minutes, respectively. The mother's routine prenatal evaluation was unremarkable and she had completed a course of corticosteroid therapy. The infant needed oxygen supplementation and was started on empirical antibiotics with intravenous (IV) ampicillin and gentamicin. Minimal enteral nutrition with breast milk was started from second day of life which was gradually increased. On day 6 of life, he needed nasal continuous positive airway pressure due to nosocomial sepsis. Antibiotics were changed to IV vancomycin and cefotaxime; feeding was stopped, and umbilical line was removed. Two days later, he had further clinical worsening with abdominal distension and decreased bowel sounds. Laboratory studies showed increased inflammatory markers (C reactive protein 24.9 mg/dL) with leucopenia (white cell count 4000/cumm). Chest and abdominal radiographs revealed signs of pneumoperitoneum, including Rigler's sign (Figure 1). An exploratory laparotomy revealed a perforation and necrosis of the cecum, ascending and transverse colon.
Figure 1. Supine radiograph of the abdomen showing the presence of air on both sides of the bowel wall (blue arrows) and infra-diaphragmatic air (white arrows)
|
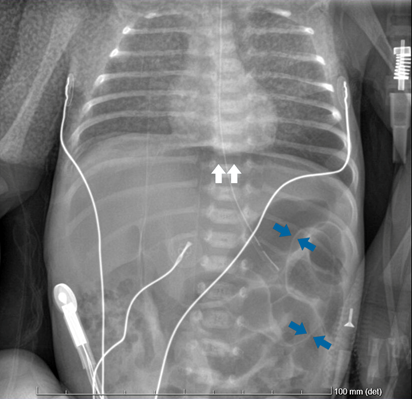
Figure 1. Supine radiograph of the abdomen showing the presence of air on both sides of the bowel wall (blue arrows) and infra-diaphragmatic air (white arrows)
|
What is Rigler's sign?
In Rigler's sign, also known as bas-relief or double wall sign, both the outer and inner walls of the bowel wall can be visualized when there is air present within the peritoneal cavity and the intestinal lumen.1,2,3,4 It is the second most common sign of pneumoperitoneum,1 seen in 14-32% of the cases.4 Presentation of this sign requires larger volume of gas and is seen most frequently in colonic and gastric perforations.4 A Rigler's sign variant occurs when only the outside of the bowel wall is visible because the lumen is filled with fluid.2,3
Optimal radiographic technique is important with a suspected abdominal perforation and at least two radiographs (a supine and a lateral decubitus in neonates) should be obtained. If Rigler's sign is believed to be present, an ultrasound or a computed tomography should be performed as well as a surgical consultation obtained.1 Early diagnosis and appropriate treatment may be lifesaving. |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Sanchez Arroyo ND, Solano JJ. Rigler Sign. [Updated 2020 Aug 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539847/
- Raturi S, Chandran S, James TE, Rajadurai VS. Radiological signs of pneumoperitoneum in an extremely low birthweight infant. BMJ Case Rep. 2014;2014:bcr2014205510. [CrossRef] [PubMed] [PMC free article]
- Ly JQ. The Rigler sign. Radiology. 2003;228:706-707. [CrossRef] [PubMed]
- Indiran V, Sivakumar V. Rigler sign. Abdom Radiol (NY). 2017;42:2588. [CrossRef] [PubMed]
- Khan, Ali N. Pneumoperitoneum imaging. Medscape Reference [Internet] 06 March 2016. [cited 07 August 2020]. Available from: http://emedicine.medscape.com/article/300901-overview
|
|
DOI: https://doi.org/10.7199/ped.oncall.2021.14 |
| |
Cite this article as:
Gonçalves C S, Fontes D, Herédia V, Mendes M J. Rigler's Sign. Pediatr Oncall J. 2021;18: 64. doi: 10.7199/ped.oncall.2021.14
|