Melissa Brigham de Figueiredo1,2, Filipa Briosa1, Joana Rios1, Paulo Oom1.
1Department of Pediatrics, Beatriz Ângelo Hospital-Loures, Portugal,
2Department of Pediatrics, São Francisco Xavier Hospital, Lisbon, Portugal.
ADDRESS FOR CORRESPONDENCE
Melissa Brigham de Figueiredo, Estrada Forte do Alto Duque, 1449-005 Lisbon, Portugal.
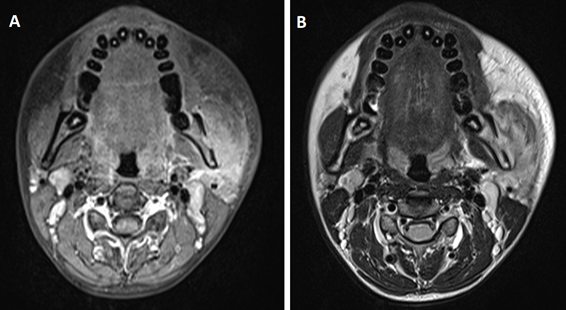
Email: brigham.figueiredo@gmail.com | | Keywords | | Actinomycosis, Actinomyces, osteomyelitis, cervicofacial mass. | | | A 16-year-old female teenager presented to the emergency department with left painful hemifacial swelling evolving over a three-month period. There was no history of trauma and she had no fever, weight loss or any other complaints. A hard, round, and painful 6 cm mandibular mass was noted, adherent to the subjacent planes. Trismus was positive. Intraoral examination was normal. Initial blood work showed mild leukocytosis (white cell count 12.41x109 cells/cumm, 70% neutrophils), an elevated sedimentation rate (38 mm/h) and mildly elevated C reactive protein (1.02 mg/dL). Cervicofacial computerized tomography and magnetic resonance imaging showed a subacute/chronic inflammatory process affecting both the masseter muscle and the mandible ramus, with bone erosion and periosteal reaction (Figure 1), along with a small amount of air on the left third molar root. Although an infectious cause was more likely, a neoplastic etiology could not be excluded. Therefore, she underwent both fine needle aspiration and ultrasound guided biopsy, which were not conclusive, showing only inflammatory cells. All cultures of the collected material and PCR for bacterial DNA and fungi were negative. Surgical biopsy of the mandible and masseter muscle was then performed, along with extraction of the third molar, and Actinomyces odontolyticus was isolated in the samples. She received intravenous amoxicillin + clavulanate and clindamycin empirically for four weeks, with clinical improvement, and switched to oral clindamycin upon isolation of A. odontolyticus. She was discharged with a regimen of oral clindamycin for 6 months and was kept on regular follow up. After 6 months, she had no palpable mass or face asymmetry.
Figure 1. MRI showing an ill-defined lesion involving the masseter muscle and the mandible, with heterogenous hypersignal in T1 (A) and anomalous hyposignal of the bone (B).
Actinomycosis is a granulomatous infectious disease caused by Actinomyces spp, filamentous gram-positive bacilli that mainly belong to the human commensal flora of the oropharynx, gastrointestinal tract, and urogenital tract.1 The infection occurs when Actinomyces penetrates through the mucosa and characteristically invades contiguous tissues, not respecting anatomic barriers and usually leading to the formation of abscesses and fistulae.2
Actinomycosis is rare, especially among the pediatric population. Cervicofacial actinomycosis is the most frequent clinical form. “Lumpy jaw syndrome” is the most common clinical presentation1, characterized by a subacute/chronic mandibular mass, usually hard and adherent, and slowly increasing in size over a period of weeks to months, reported by this patient. Predisposing conditions include poor oral hygiene and oral mucosa trauma.1,2,3 Actinomyces infections pose a diagnostic challenge, especially because they must be distinguished from neoplastic etiologies and other infections. In most reported cases in the literature, actinomycosis is not suspected at the clinical onset of symptoms.2,3 However, an early diagnosis is important, since it is a treatable condition and prompt diagnosis can avoid potentially unnecessary workup and intervention.4 Also, Actinomyces’ growth is very fastidious, and microbiological diagnosis often requires prolonged incubation times (up to 21 days).4
Effective treatment of actinomycosis often requires both surgical management and prolonged antibiotic therapy.1,2,3,4 Actinomyces species are universally susceptible to penicillin, amoxicillin and clindamycin, and a 4–6 weeks high-dose parenteral regimen is usually recommended followed by 2-12 months of oral penicillin4 or clindamycin.
Despite its low prevalence in childhood and adolescence, this case enlightens the importance of considering actinomycosis in the differential diagnosis of subacute/chronic cervicofacial masses in the pediatric population.
| | | | Acknowledgement | - Carlos Macor, Otorhinolaryngology Consultant; Otorhinolaryngology Department, Beatriz Ângelo Hospital – Loures, Portugal.
- António Gonçalves, Radiology Consultant; Radiology Department, Beatriz Ângelo Hospital – Loures, Portugal. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Valour F, Sénéchal A, Dupieux C, Karsenty J, Lustig S, Breton P, et al. Actinomycosis: Etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014;7:183-197. [CrossRef] [PubMed] [PMC free article]
- Bonnefond S, Catroux M, Melenotte C, Karkowski L, Rolland L, Trouillier S, et al. Clinical features of actinomycosis: A retrospective, multicenter study of 28 cases of miscellaneous presentations. Medicine (Baltimore) [Internet]. 2016;95:e3923. [CrossRef] [PubMed] [PMC free article]
- Sama CB, Mbarga NF, Oben CE, Mbarga JA, Nfor EK, Angwafo Iii FF. Massive paediatric cervicofacial actinomycoses masquerading as an ulcerative malignancy. BMC Infect Dis. 2016;16:417. [CrossRef] [PubMed] [PMC free article]
- Thacker SA, Mary Healy C. Pediatric cervicofacial actinomycosis: An unusual cause of head and neck masses. J Pediatric Infect Dis Soc. 2014;3:e15-19. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2022.1
|
| Cite this article as: | | Figueiredo M B d, Briosa F, Rios J, Oom P. A Case of Lumpy Jaw Syndrome In A Teenage Girl. Pediatr Oncall J. 2022;19: 27-28. doi: 10.7199/ped.oncall.2022.1 |
|