Andreia Romana1, Maria Filomena Cardosa1, Cristina Lorenzo2, Joana Matias1, Marta Almeida1, Paulo Calhau1.
1Department of Pediatrics, Hospital Garcia de Orta, Almada, Portugal,
2Department of Pediatrics, Hospital de Santa Maria - Centro Hospitalar Universitário de Lisboa Norte, EPE, Lisboa, Portugal.
ADDRESS FOR CORRESPONDENCE
Andreia Romana, Avenida Torrado da Silva, 2805-267 Almada, Portugal.
Email: andreiascromana@gmail.com | | Abstract | Introduction: Complex chronic conditions are becoming more prevalent in paediatric age, as a group of diseases requiring a multiplicity of care and technological resources and with a great impact on children, family and society. Palliative care has a growing significance in its approach.
Methods: Observational, longitudinal and retrospective analysis of hospital admissions due to complex chronic conditions in the Paediatric Ward of a level II hospital over a five-year-period (2015-2019).
Results: We had 431 hospitalizations (209 patients), corresponding to 18% of total hospital admissions in the period studied. Median length of stay was 5 days. Male sex counted for 59% of all hospitalizations and median age was 5 years. The most frequent categories were neurologic and neuromuscular disorders (39%) and hematologic disorders (23%); the main diagnosis were sickle cell disease (23%) and cerebral palsy (16%). We verified pluripathology in 15% and polymedication in 32%. The most associated comorbidities were epilepsy (29%) and sleep disorders (18%). Dependency on technological support was found in 26%. The decompensation of the underlying disease was the main reason for hospitalization (52%); 4 hospitalizations were aimed to caregiver’s rest. 14% of patients had ambulatory’s specific support. Death occurred in 4 patients.
Conclusion: This study, innovative at national level, revealed a significant rate of hospital admissions due to complex chronic conditions. Awareness of this reality is essential for planning a suitable healthcare system based on a multidisciplinary approach. It is crucial to encourage our national Paediatric Palliative Care network and enhance education and social security support.
| | | | Keywords | | Complex chronic conditions, Paediatric palliative care, Holistic approach | | | | Introduction | Complex Chronic Conditions (CCC) include a set of clinical conditions that are increasingly prevalent in paediatric age, due to remarkable advances in paediatric healthcare and technological evolution in the last decades. These factors have decisively contributed to a longer survival in this group of patients.1
The concept of CCC comprises disease’s evolution time and its impact on the child.2 Feudtner et al defined CCC as “any medical condition that can be reasonably expected to last at least 12 months (unless death intervenes) and to involve either several different organ systems or one organ system severely enough to require specialized paediatric care and probably some period of hospitalization in a tertiary care center”.3
CCC’s prevalence among children and adolescents in Portugal is not well known. A recent study analyzed paediatric mortality in our country between 1987 and 2011 and concluded that there were 10571 deaths from CCC, corresponding to 27% of paediatric mortality in this period.4 Another study, published in 2019, revealed that 15.5% of paediatric hospital admissions in mainland Portugal between 2011 and 2015 corresponded to patients with at least one CCC’s cathegory.5 These data suggest a significant prevalence of CCC in paediatric age in Portugal.
CCC are severe organic diseases, most of them without cure, which require a multiplicity of care, technological and therapeutic resources and frequent need for hospitalization.
Palliative care is crucial for an adequate CCC’s management. According to the Association for Children’s Palliative Care, paediatric palliative care offers an active and comprehensive approach and management to children and adolescents from initial diagnosis, throughout life and after death.6 It focuses on improving patient’s and caregivers’ well-being and family support covering physical, emotional, social and spiritual dimensions.
According to the World Health Organization, main objectives of palliative care include prevention and relief of suffering of paediatric patients and their families, that are confronted with multiple issues derived from a life-threatening disease.7 Palliative care is thus considered a basic human right for all children, in particular for CCC carriers.8 Amelioration of quality of life and minimizing pain and distress through an integrated and multidisciplinary approach must be the goal.9,10
This study aimed to characterize level II hospital admissions of children and adolescents with CCC through socio-demographic analysis, identification of main disorders and comorbidities, characterization of hospitalizations and ambulatory care follow-up. | | | | Methods & Materials | Observational, longitudinal and retrospective analysis of hospital admissions due to CCC in the Paediatric Ward of a level II hospital over a five-year period (from January 1st, 2015, to December 31st, 2019).
Definitions and Concepts
We used Feudtner et al CCC’s definition published in 2000 and updated in 2014, which includes ten CCC categories: neurologic and neuromuscular, cardiovascular, respiratory, renal and urologic, gastrointestinal, hematologic or immunologic, metabolic, other congenital or genetic defects, malignancy, premature and neonatal.1,3 Two aspects of this classification were included, independent from the above-mentioned categories: technological dependency and organ transplantation.1,3
For categorization of CCC we used the diagnostic codes of the International Statistical Classification of Diseases and Related Health Problems, version 10 (ICD-10).
We defined pluripathology as the occurrence of two or more CCC categories in the same patient and main CCC as the disease with the greatest impact on quality of life and suffering of the child.
Polymedication was designated as the daily use of three or more drugs.
We considered a social case as the situation in which hospital discharge was deferred to ensure a formal support network that guaranteed the continuity of care after hospital discharge, or whenever the complexity of social and environmental situation had the potential to worsen biological and psychological health conditions.11
Readmission was defined as the need for rehospitalization due to the same disease and up to 30 days after hospital discharge.
Sample Selection
Our sample included patients with CCC aged from 0 to 17 years and 364 days old that were admitted in the Paediatric Ward in the above-mentioned 5-year-period.
Data Collection
Data was collected retrospectively by consulting patients’ electronic clinical files. We obtained information about socio-demographic parameters (age, gender, educational insertion, place of residence); main caregiver (age, academic qualifications); household (type of family); CCC characterization (category, age of diagnosis, evolution, presence of comorbidities, polymedication, need for technological support, outpatient follow-up, do-not-resuscitate order - dnr); characteristics of hospital admissions (date, cause, duration, readmissions, death), including the annual number of hospitalizations per patient. We assigned a code for each hospital admission in our database to ensure anonymization.
Data Analysis
We performed a descriptive analysis of all sociodemographic variables and CCC’s hospital admissions. Data was analyzed using Microsoft Excel 2011® program.
| | | | Results | We had 431 hospital admissions for CCC (209 patients), corresponding to 18% of the paediatric hospital admissions in the studied period (n=2405).
Sociodemographic Characterization
Male sex counted for 59% of all hospitalizations. Median age was 5 years in the child’s first hospitalization (minimum 0 – maximum 17); of all patients, 54% were younger than 5 years (30% ≤12-month-old) (Figure 1).
Figure 1. Distribution of patients by age
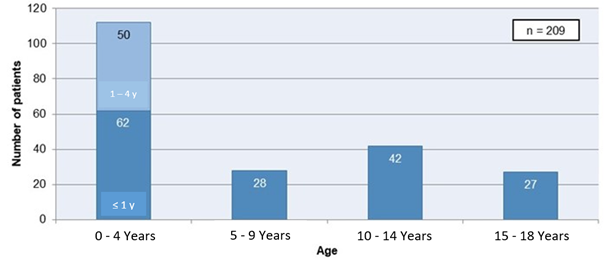
Regarding educational integration, 59% of our patients attended school, 3% were integrated in care centers and 1% in institutions; 37% did not make part of an educational facility of any sort.
As for the area of residence, nearly all patients lived in Lisbon metropolitan area (96%); 2% resided in Alentejo, 1% in the Central Region and 1% in the autonomous region of the Azores. Almost all patients lived at home (99%) and three patients were institutionalized (1%).
We verified a median age of the primary caregiver of 39 years in the child’s first hospitalization (minimum 16 – maximum 53), most of them ranging from 30- to 50-year-old (n=137); 49 were younger than 30 years old and four of them over 50; there was no data concerning the age of 19 caregivers (9%).
Regarding main caregiver’s academic qualifications, 72 caregivers had completed higher education, 42 completed secondary and 23 primary education and 1 caregiver had no academic qualification. We could not obtain data concerning this parameter in 71 cases (34%).
Most children were part of a nuclear family (n=159), while 34 children belonged to single-parent family and 1 child to an extended family. Household data was missing in 15 cases (7%).
CCC Characterization
Most frequent CCC categories were (Table 1):
• neurologic and neuromuscular (39%), mainly cerebral palsy (n=68) and neurogenetic syndromes (n=36);
• hematologic or immunologic (23%), all of them sickle cell disease (n=100);
• other congenital or genetic defects (13%), of which Down syndrome was the most prevalent (n=12);
• neonatal and premature (7%), with 14 hospitalizations due to bronchopulmonary dysplasia.
Table 1. Distribution of hospitalizations by CCC categories.
| CCC Categories |
n |
Percentage |
| Neurologic and neuromuscular |
168 |
39% |
| Hematologic or immunologic |
100 |
23% |
| Other congenital or genetic defect |
58 |
13% |
| Premature and neonatal |
30 |
7% |
| Malignancy |
19 |
4% |
| Renal or urologic |
19 |
4% |
| Cardiovascular |
12 |
3% |
| Metabolic |
10 |
2% |
| Gastrointestinal |
8 |
2% |
| Respiratory |
7 |
2% |
Most frequent diseases were sickle cell disease (23%), cerebral palsy (16%) and neurogenetic syndromes (8%).
Pluripathology was present in 64 hospital admissions (15%). Within this subgroup of patients, most frequent secondary CCC categories were:
• neonatal and premature (n=22), with bronchopulmonary dysplasia being the most common diagnosis (n=15);
• neurologic and neuromuscular (n=14), of which cerebral palsy is highlighted (n=11);
• cardiovascular diseases (n=14), mostly due to congenital heart defects (n=8).
Other secondary CCC were malignancy (n=3), respiratory (n=2), renal and urologic (n=1), hematologic or immunologic (n=1) and metabolic (n=1).
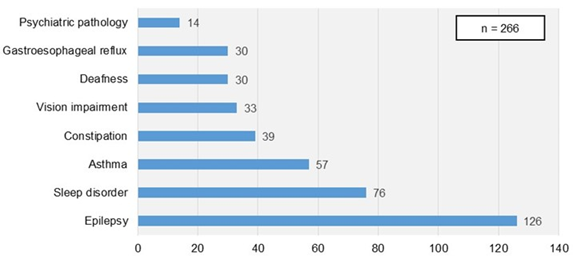
Comorbidities were present in 266 (62%) of all hospital admissions (in 176 cases more than one comorbidity was detected). Most frequent comorbidities were epilepsy (29%), sleep disorders (18%) and asthma (13%) (Figure 2).
Figure 2. Associated comorbidities in hospitalized patients with CCC.
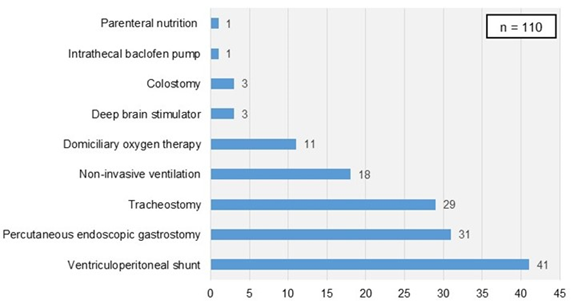
Technological dependency was present in 112 hospitalizations (26%), of which 87 cases had a single-organ support dependency (Figure 3). The most frequent technological support was ventriculoperitoneal shunt (n=41), followed by endoscopic percutaneous gastrostomy (n=30) and tracheostomy (n=29).
There were no hospitalizations due to organ transplantation.
Figure 3. Technological support in hospitalized patients with CCC.
Regarding CCC’ time of diagnosis, we found a median age of 3-months. Antenatal diagnosis occurred in 21 patients (10%) and in neonatal period in 86 patients (41%); in most cases, diagnosis was made in the first year of life (72%).
Median time from diagnosis to first hospitalization was three years.
Polymedication was present in 52 patients (25%) and 138 hospitalizations (32%), predominantly in children and adolescents with neurologic and neuromuscular (n=78) and hematologic or immunologic diseases (n=30).
Regarding ambulatory care, 14% of patients had specific support, most of them (18/29) had a regular follow-up in our hospital’s Paediatric Palliative Care team (Equipa Intra Hospitalar de Suporte em Cuidados Paliativos Pediátricos - EIHSCPP); patients that were not assisted by this team had social support (n=7), psychological support (n=2) and Integrated Continuing Care team support (ICC, n=2). dnr was registered in 2% of all hospital admissions (six hospitalizations corresponding to four children).
Hospital admissions’ characterization
We had a median of annual hospital admissions of 86 (minimum 79 – maximum 92) and 1 hospitalization per patient (minimum 1 – maximum 16). Median hospital stay was 5 days (minimum 1 -maximum 210), which was longer when compared with non-CCC hospitalizations (median of 3 days).
CCC’s complications were responsible for 52% of hospital admissions, followed by infections (17%), respiratory or neurologic causes (15% and 7%, respectively), technological support dysfunction (5%), need for nutritional support (3%) and caregiver’s rest (1%; n=4).
Social cases were identified in 4% of all hospitalizations (n=15), corresponding to five patients.
Hospital readmissions occurred in 17% of cases (n=73), mostly motivated by CCC’s complications (n=37); about half of them occurred in patients with neurologic and neuromuscular diseases (n=35). In the same five-year-period, number of readmissions in the Paediatric Ward for any reason was 133.
There were four deaths (1% of all hospitalizations). In three children death occurred as a consequence of a low-respiratory infection: 9- and 14-year-old children with cerebral palsy and a 10-year-old child with Down syndrome. The fourth death occurred in a six-month-old infant who had a congenital glycosylation disorder, in the context of refractory status epilepticus. dnr was only registered in two of them (50%). | | | | Discussion | The significant improvement in the extent and quality of medical care in recent decades, although asymmetrically on a global scale, has contributed to a significant decrease in paediatric mortality, which is currently low in developed countries. As a result of the improvement in paediatric morbidity and mortality, chronic disease in paediatric age has emerged in a greater dimension, leading to new challenges for patients, families and caregivers, communities and national healthcare systems.
Patients with CCC require a multidisciplinary follow-up, in ambulatory and hospital setting and have multiple and permanent needs; nevertheless, health institutions are not yet sufficiently prepared to face them. On the other hand, the emotional, affective, work productivity and absenteeism and financial impact that these patients have on their families is of outstanding relevance, often framed in a society that is still poorly prepared and attentive to their needs.
This is an innovative study at a national level, which revealed a significant number of hospitalizations in children and adolescents due to CCC, representing 18% of total paediatric hospital admissions in a level II hospital over a five-year-period. This value is similar to what was reported in two studies, at both national level (15.5% of paediatric hospitalizations corresponded to patients with at least one category of CCC, according to Lacerda et al.5) and international level (prevalence of 13% to 18% for CCC hospital admissions in Canada).12
Other studies carried out in Brazil13 and in the United States14, demonstrated a prevalence of approximately 10%, a lower value if compared to what we found in our study. This may be related, among other factors, to the different diagnostic codification, sample differences and different access to healthcare.
The median age in our study was five years, which is higher than the median age reported in a study performed at the CCC Unit of Hospital Universitario La Paz, which was two years.15
The greater number of hospitalizations in the first five years of life was also reported by Newacheck et al.16 and may be related not only with the higher frequency of decompensation of CCC and infectious diseases, which are the predominant causes of hospital admissions, but also with caregiver’s insecurity in managing these complications at home during the first years of their child’s life and disease.
According to other studies15,16,17, we also verified a predominance of male patients (59%). This reflects the greater need for specialized health care between male children and adolescents, who often have a more severe disease.16
Most children lived in municipalities which belong to the hospital catchment area or in neighboring municipalities. Only 4% of patients lived in other regions of the country but had a regular outpatient Neurosurgery and paediatric Neurology follow-up in our hospital.
Regarding main caregiver sociodemographic characterization, we observed that most caregivers were between 30–50-year-old and that many had completed secondary school or had higher academic qualifications; these two aspects could have a positive impact on children with CCC, as they may reflect a greater CCC and palliative care literacy. However, a significant number of caregivers had only completed basic education and one caregiver had none, a factor that may increase the vulnerability of this population and quality of care provided, as their access to medical information could be limited.
Concerning social, family and school context, most children and adolescents were inserted in a nuclear family and were integrated in schools, fact that promote a more cohesive intrafamily support and a better social integration. Nevertheless, a significant number of patients belonged to single-parent household, which may increase the risk of social vulnerability of the child and his/her caregiver. This could have a direct impact on quality of life and, possibly, life expectancy. CCC implies an enormous burden, multiplicity of care and frequent hospitalizations; social precariousness on which some of these families find themselves will inevitably hinder the management of the disease which, per se, is already considerably difficult and complex.
In our study, CCC diagnosis was made in the first year of life in most cases. Early-age diagnosis is essential as it allows a prompt beginning of care and a timely multidisciplinary follow-up.
The most frequent CCC categories were neurologic and neuromuscular, hematologic or immunologic and congenital or other genetic diseases. These results are in relation with the Paediatric Service´s differentiation in the areas of Development, Paediatric Neurology and Neonatology. The higher prevalence of hematologic CCC category can be explained by the high prevalence of sickle cell disease in the population of the hospital catchment area.
Pluripathology was identified in 15% of all hospitalizations, a lower percentage when compared to other studies15; this result is perhaps explained by missing data in patient’s electronic clinical files and differentiated recruitment of patients and pathologies among several of the institutions evaluated in these studies. In our study, premature and neonatal diseases were the most frequent secondary diseases, in agreement with the higher prevalence of hospitalizations of children in the first years of life and at early stages of adaptation to their disease.
One or more associated comorbidities were verified in most hospitalizations, with a higher prevalence of epilepsy and sleep disorders. Polymedication need was observed in approximately one third of hospitalizations, mainly detected in patients with neurologic and neuromuscular and hematologic and immunologic diseases.
Dependency on technological support was detected in 26% of all hospitalizations. It is a lower value if compared with other studies carried out in tertiary hospitals or specialized CCC Units, such as the study by Alcalá et al. from the CCC Unit of Hospital Universitario La Paz (Madrid), with 69% of patients being technologically dependent.15 In our study, which was conducted in a less differentiated hospital of CCC, were also included some patients with more complex technological dependency, such as intrathecal baclofen pump or deep brain stimulator. Nevertheless, the most frequent technological support for symptomatic and functional improvement was ventriculoperitoneal shunt system, which is related to the high prevalence of neurologic disease observed.
Median hospital stay in our study was five days, which is significantly higher than the median duration of all paediatric hospitalizations in the same period. However, this value is lower than what is considered in some studies as “long-term hospitalization” (minimum of 10 days); longer hospital stays are usually associated with respiratory CCC18, a less frequent category found in this study.
On the other hand, it is worth mentioning that our working model focuses on outpatient care (visit and in-home care, post-discharge assessment at day hospital care). We would like to highlight the case of an infant with Kagami-Ogata syndrome, a rare genetic disease, who were hospitalized for 210 days; discharged was deferred until the child's clinical situation and home conditions were fully met, including caregiver’s confidence and ability to provide proper care.
The main cause for hospitalization were complications of the primary CCC. Only four hospital admissions were made to promote family’s balance and organization due to caregiver’s exhaustion, which are fundamental aspects of an adequate support policy to CCC patients and families.19 However, it should be noted that in all hospitalizations, caregiver’s rest was encouraged and actively coached by the health teams. In fact, this strategy is essential for an adequate management of physical, emotional and social burden associated to the complexity of children with these diseases, who most often have their mother as the main caregiver.20
The annual hospitalization rate due to CCC remained stable over the five-year-period, which could be correlated not only with the scientific and technological progress that allowed a greater symptomatic control, but also with the creation of the EIHSCPP in 2017, which is responsible for promoting support care to patients and families. However, only about one fifth of hospitalizations had specific ambulatory care support; therefore, timely referral to both EIHSCPP and community care teams should be a priority.
We observed a substantial proportion of readmissions (17%), which represents more than three times those that occurred in all paediatric hospitalizations in the same period. This is a direct consequence of the complexity of the underlying disease, associated complications and comorbidities.21 Although many authors consider readmission rate as a marker to assess the quality of hospital care22,23, we believe that understanding what is behind this metric is crucial to create measures which may result in a lower number of potentially avoidable readmissions.
The reduced number of dnr records on clinical files is probably explained by the omission of the registration of that decision in our electronic files and due to the absence of a timely decision. It is essential to periodically review an individualized care plan with the family and to anticipate, when possible, the most probable disease’s evolution in patients with CCC. Once dnr decision may be indicated, this decision should be discussed between the health team and the main caregiver, ideally in the non-terminal phase of the disease, as to avoid taking this decision abruptly or under pressure. We want to emphasize the importance of the registration of this decision in the patient’ clinical file, in a clear and unambiguous manner, stating the end of life’s care measures desired by the family and, eventually, the patient.
Palliative care serves many purposes such as survival increase, quality of life and daily symptoms’ improvement, reduction of the need of hospital admissions and patient and caregiver greater well-being.24 Several models have been suggested regarding CCC paediatric patients, often centered on the families, focused in promoting the acquisition of self-care skills and emphasizing close relations with health teams.25,26,27,28
With this study, we intend to increase our knowledge about CCC paediatric population and so to improve the quality of life of these children and families, by promoting palliative care and social integration.
This work has two main limitations. First, it is a retrospective study, a factor that impairs access to data. Additionally, this study was conducted on a single institution, a level II hospital, so it may not be representative of the Portuguese reality and generalizable to our paediatric population. | | | | Conclusion | This study allowed us to conclude that medically complex patients constitute an important percentage of all paediatric hospitalizations. Children and adolescents with CCC are a significant part of hospital care, requiring appreciable human, technological and financial resources. They represent a population with higher and longer hospitalizations, also in intensive care units, with greater need for technological support and differentiated healthcare professionals.
Awareness of this reality at local and national level is essential for a multidisciplinary, coordinated and sustainable health care provision (hospital and ambulatory care), as well as in other areas, as educational and social support. We are constantly being confronted by CCC paediatric patients and their families with legitimate expectations and demands. Healthcare professionals and policy makers must be particularly committed to the design and implementation of the most appropriate healthcare models for these patients, whose incidence has been increasingly growing in the last years worldwide.
The implementation of paediatric palliative care teams on a national scale is still a recent reality in our country, which needs to be encouraged, supported and developed. Development and creation of specialized CCC units in tertiary-level hospitals is crucial, together with the adaptation of level II hospital services to meet this population’s needs.
Communication between family, healthcare professionals, paediatric palliative care team and community support network is a fundamental component in all phases of the disease’s evolution.
| | | | Financial Disclosure | | The authors have no financial relationships relevant to this article to disclose. | | | | Compliance with Ethical Standards | | Funding | | There were no external funding sources for the realization of this paper. | | | | Conflict of Interest None | | |
- Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatrics. 2014;14:199 [CrossRef] [PubMed] [PMC free article]
- Perrin EC, Newacheck P, Pless IP, Drotar D, Gortmaker SL, Leventhal J, et al. Issues involved in the definition and classification of chronic health conditions. Pediatrics. 1993;91:787-93 [CrossRef] [PubMed]
- Feudtner C, Christakis DA, Connell FA. Pediatric deaths attributable to complex chronic conditions: a population-based study of Washington State, 1980-1997. Pediatrics. 2000;106:205-9. [CrossRef] [PubMed]
- Lacerda AF, Gomes B. Trends in cause and place of death for children in Portugal (a european country with no paediatric palliative care) during 1987-2011: a population-based study. BMC Pediatrics. 2017;17:215 [CrossRef] [PubMed] [PMC free article]
- Lacerda AF, Oliveira G, Cancelinha C, Lopes S. Utilização do internamento hospitalar em Portugal continental por crianças com doenças crónicas complexas (2011 - 2015). Acta Médica Portuguesa. 2019;32(7-8):488-98 [CrossRef] [PubMed]
- Downing J, Kiman R, Boucher S, Nkosi B, Steel B, Marston C, et al. Children's palliative care now! Highlights from the second ICPCN conference on children's palliative care, 18-21 May 2016, Buenos Aires, Argentina. ecancer. 2016; 10:667 [CrossRef] [PubMed] [PMC free article]
- World Health Organization. Integrating palliative care and symptom relief into paediatrics: a WHO guide for health care planners, implementers and managers. 2018.
- The United Nations. Convention on the rights of the child. Treaty Series. 1989. 1577:3.
- Himelstein BP, Hilden JM, Boldt AM, Weissman D. Pediatric palliative care. New England Journal of Medicine. 2004;350:1752-62 [CrossRef] [PubMed]
- Michelson KN, Steinhorn MD. Pediatric end-of-life Issues and palliative care. Clinical Pediatric Emergency Medicine. 2007;8(3): 212-19 [CrossRef] [PubMed] [PMC free article]
- Guerra, I. O que é o caso social? Estudo sobre a construção do caso social em contexto hospitalar. Tese de Doutoramento em Serviço Social, Lisboa, Faculdade de Ciências Humanas, Universidade Católica Portuguesa; 2015
- Bethell CD, Read D, Blumberg SJ, Newacheck P. What is the prevalence of children with special health care needs? Toward an understanding of variations in find¬ings and methods across three national surveys. Maternal and Child Health Journal. 2008; 12(6):1-14 [CrossRef] [PubMed]
- Moura EC, Moreira MCN, Menezes LA, Ferreira IA, Gomes R. Complex chronic conditions in children and adolescents: hospitalizations in Brazil, 2013. Ciência & Saúde Coletiva. 2017;22(8):2727-34 [CrossRef] [PubMed]
- Simon TD, Berry J, Feudtner C, Stone BL, Sheng X, Bratton SL, et al. Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics. 2010;126:647-55 [CrossRef] [PubMed] [PMC free article]
- Alcalá FJC, Villalta MGF, García LE, Alonso AR, Velasco LAA. Unidad de niños con patología crónica compleja. Un modelo necesario en nuestros hospitales. Anales de Pediatria. 2018;88(1):12-18 [CrossRef] [PubMed]
- Newacheck PW, Kim SE. A national profile of health care utilization and expenditures for children with special health care needs. Archives of Pediatric Adolescent Medicine. 2005;159(1):10-17 [CrossRef] [PubMed]
- López M, Fernández A, Fiquepron K, Meregalli C, Ratto M, Serrate A. Prevalence of children with complex chronic conditions in PICUs of Argentina: A prospective multicenter study. Pediatric Critical Care Medicine. 2020; 21(3):e143-e151 [CrossRef] [PubMed]
- Gold JM, Hall M, Shash SS, Thomson J, Subramony A, Mahant S, et al. Long length of hospital stay in children with medical complexity. Journal of Hospital Medicine. 2016. 00:1-7
- Allshouse C, Comeau M, Rodgers R, Wells N. Families of children with medical complexity: a view from the front lines. Pediatrics. 2017. 141(3):196-201 [CrossRef] [PubMed]
- Cohen E, Berry JG, Sanders L, Schor EL, Wise PH. Status Complexicus? The emergence of pediatric complex care. Pediatrics. 2018;141(3):203-11 [CrossRef] [PubMed]
- Wijlaars LPMM, Gilbert R, Hardelid P. Chronic conditions in children and young people: learning from administrative data. Archives of Disease in Childhood. 2016; 101 (10):881-5 [CrossRef] [PubMed] [PMC free article]
- Nakamura MM, Toomey SL, Zaslavsky AM, Berry JG, Lorch SA, Jha AK, et al. Measuring pediatric hospital readmission rates to drive quality improvement. Academic Pediatrics. 2014;14(5):S39-46 [CrossRef] [PubMed]
- Srivastava R, Keren R. Pediatric readmissions as a hospital quality measure. Journal of the American Medical Association. 2013;309(4):396-8 [CrossRef] [PubMed]
- Kavalieratos D, Corbelli J, Zhang D, Dionne-Odom N, Ernecoff NC, Hanmer J, et al. Association between palliative care and patient and caregiver outcomes - a systematic review and meta-analysis. JAMA. 2016;316(20):2104-14 [CrossRef] [PubMed] [PMC free article]
- Kuo DZ, McAllister JW, Rossignol L, Turchi RM, Stille C. Care coordination for children with medical complexity: whose care is it, anyway? Pediatrics. 2018. 141(3):225-32 [CrossRef] [PubMed]
- Noritz G, Madden M, Roldan D, Wheeler A, Conkol K, Brilli R, et al. A population intervention to improve outcomes in children with medical complexity. Pediatrics. 2017. 139(1):2-10 [CrossRef] [PubMed]
- Cohen E, Kuo DZ, Agrawal R, Berry JG, Bhagat KM, Simon TD, Srivastava R. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. 2011. 127(3):529-38 [CrossRef] [PubMed] [PMC free article]
- Newacheck PW, Rising JP, Kim SE. Children at risk for special health care needs. Pediatrics. 2006; 118 (1):334-42 [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2023.9
|
| Cite this article as: | | Romana A, Cardosa M F, Lorenzo C, Matias J, Almeida M, Calhau P. Pediatric Department Hospital admissions due to Complex Chronic Conditions: A Retrospective Study. Pediatr Oncall J. 2023;20: 1-7. doi: 10.7199/ped.oncall.2023.9 |
|