Vishwaraj C R1, Kavitha S2, Rengaraj Venkatesh3, Lavanya Gottigere Shankar4.
1Medical Consultant, Glaucoma Services, Aravind Eye Hospital, Pondicherry, India,
2Head of Department, Glaucoma Services, Aravind Eye Hospital, Pondicherry, India,
3Chief Medical Officer, Aravind Eye Hospital, Pondicherry, India,
4Fellow in Paediatric Ophthalmology, Aravind Eye Hospital, Pondicherry, India.
ADDRESS FOR CORRESPONDENCE
Dr. Kavitha Srinivasan, Aravind Eye Hospital, Pondicherry-605007, India.
Email: skavitha.shree@gmail.com. | | Abstract | Aim: To report a case of persistent pupillary membrane and secondary angle closure glaucoma in a child.
Summary: An 11-year old boy presented with decreased vision in right eye (RE). His visual acuity was 1/60 in RE, 6/6 in left eye (LE). On examination he had larger cornea, brownish strands of tissue arranged in a cartwheel pattern suggestive of persistent pupillary membrane (PPM) in pupillary area in RE. His intraocular pressure (IOP) was 54mm Hg in RE (Normal: 10-21mm Hg), 16mm Hg in LE. He was started on topical anti-glaucoma medications in RE. He underwent Trabeculectomy in RE as IOP could not be controlled medically. Though IOP normalized vision loss could not be reversed.
Conclusion: Routine visual acuity testing and eye examination in paediatric age group will help in early diagnosis of rare cases like PPM and can help in preventing visual compromise due to amblyopia and glaucoma
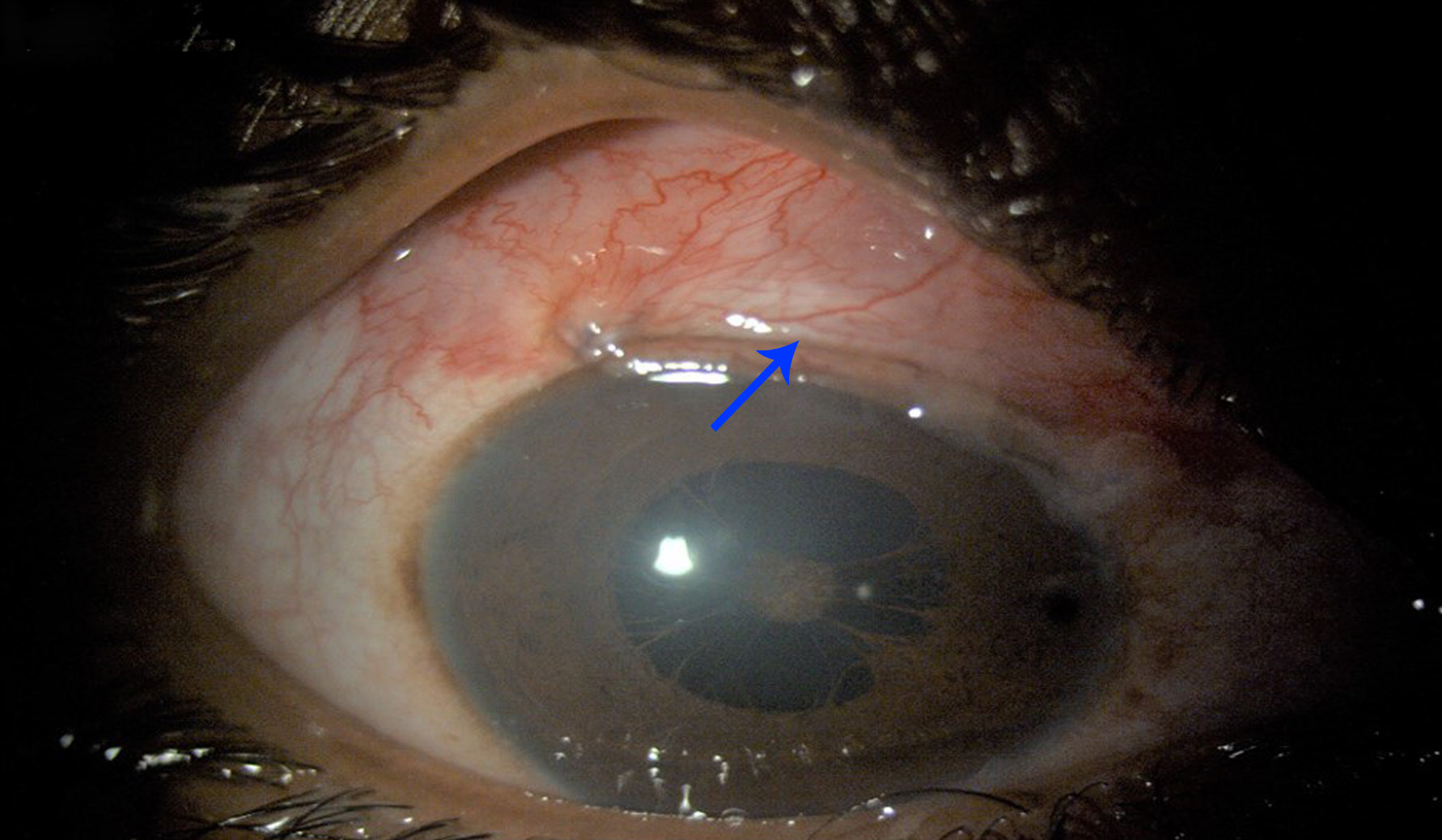
| | | | Keywords | | Paediatric Glaucoma, Persistent Pupillary, Membrane, Amblyopia, Intraocular Pressure. | | | | Introduction | | Persistent pupillary membrane (PPM) represents a relatively common congenital ocular anomaly seen in 95% of neonates and 20% of adult population1 that appears as fine iris strands along the pupil. It is a remnant of anterior tunica vasculosa lentis that supplies nutrition to the lens in fetal life. Although most cases are sporadic and incidental without any other co-morbidities, it is rarely associated with certain conditions like Hallermann-Streiff syndrome, Donnai-Barrow Syndrome and Aicardi’s syndrome.2 It can lead to amblyopia (reduced vision in the eye caused by abnormal visual development early in life). Glaucoma has been reported rarely in PPM.3 Glaucoma is a chronic, progressive, multifactorial optic neuropathy which damages the optic nerve with resultant irreversible loss of visual function. Worldwide, glaucoma is the most common cause of irreversible blindness in adults and one of the leading causes of blindness in children.4 Paediatric glaucomas can be either primary or secondary. Primary glaucomas are congenital and can be associated with syndromes whereas secondary glaucomas are associated with other ocular comorbidities like uveitis, congenital cataract surgery. The prevalence of primary congenital glaucoma (PCG) is one in 3,300 live births and PCG accounts for 4.2% of all childhood blindness in Indian population.5 We report a rare case of unilateral persistent pupillary membrane with secondary glaucoma in a child. | | | | Case Report | An 11 year old boy presented to our primary eye care centre with defective vision in right eye (RE), which he realized accidentally while closing his left eye (LE). He was noted to have high intraocular pressure (IOP) and was referred to the glaucoma department at the base hospital for further evaluation. On examination he had a best corrected visual acuity of 1/60 in RE and 6/6 in LE. Anterior segment evaluation showed redness, increased size of the cornea compared to LE, brownish strands of tissue covering the pupil, arranged in a cart wheel manner suggestive of persistent pupillary membrane (PPM), clear lens in RE (Figure 1). His LE was normal. His intraocular pressure (IOP) measured with Goldmann applanation tonometry was 54mm Hg in RE, 16 mm Hg in LE (Normal IOP range 10-21mm Hg). Gonioscopy which is used to assess the angle morphology of the eye (aqueous humor outflow pathway) showed open angles with intermittent peripheral anterior synechiae (PAS) which is adhesion of the peripheral iris to the cornea obstructing the outflow, in 3 quadrants in RE (Figure 2), normal open angles in LE (Figure 2). Fundus evaluation showed advanced glaucomatous damage (cup disc ratio of 0.9) in RE optic nerve head, LE was normal with a cup disc ratio of 0.3 (Figure 3). Visual field examination was not possible due to poor visual acuity in RE. He was started on medical therapy in RE however IOP could not be controlled with maximum possible medical therapy including timolol, brimonidine, dorzolamide and latanoprost. Considering the advanced stage of the disease and medically uncontrolled IOP he was advised trabeculectomy in RE in order to prevent painful blind eye. The surgery was uneventful with a good filtering bleb (Figure 4). His vision in the right eye did not improve as the optic nerve head damage caused by glaucoma is irreversible. He is being followed up regularly and his IOP is maintaining well within the normal limits without any antiglaucoma medications for the past 1 year.
Figure 1. Slit lamp photography, showing Persistent Pupillary Membrane in right eye, note a normal left eye.
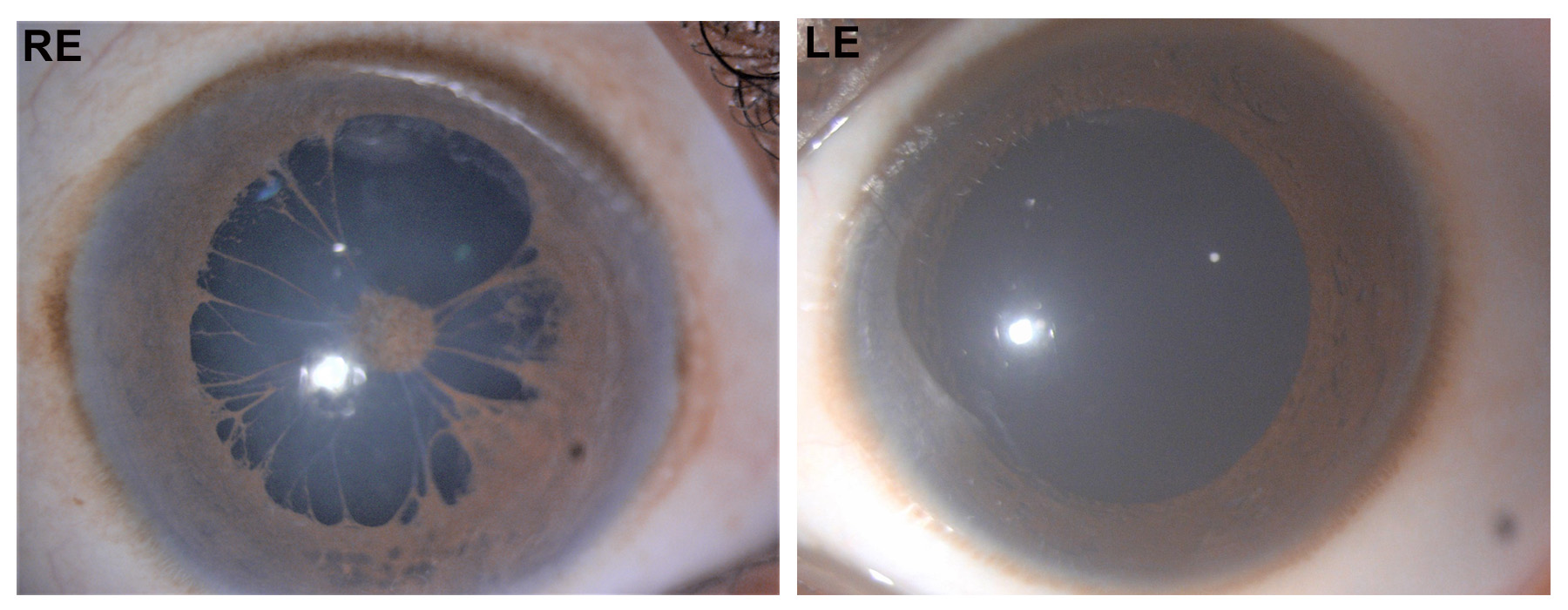
Figure 2. Gonioscopic image of the right eye showing peripheral anterior synechiae (blue arrow), note normal outflow pathway (red arrow) in left eye.
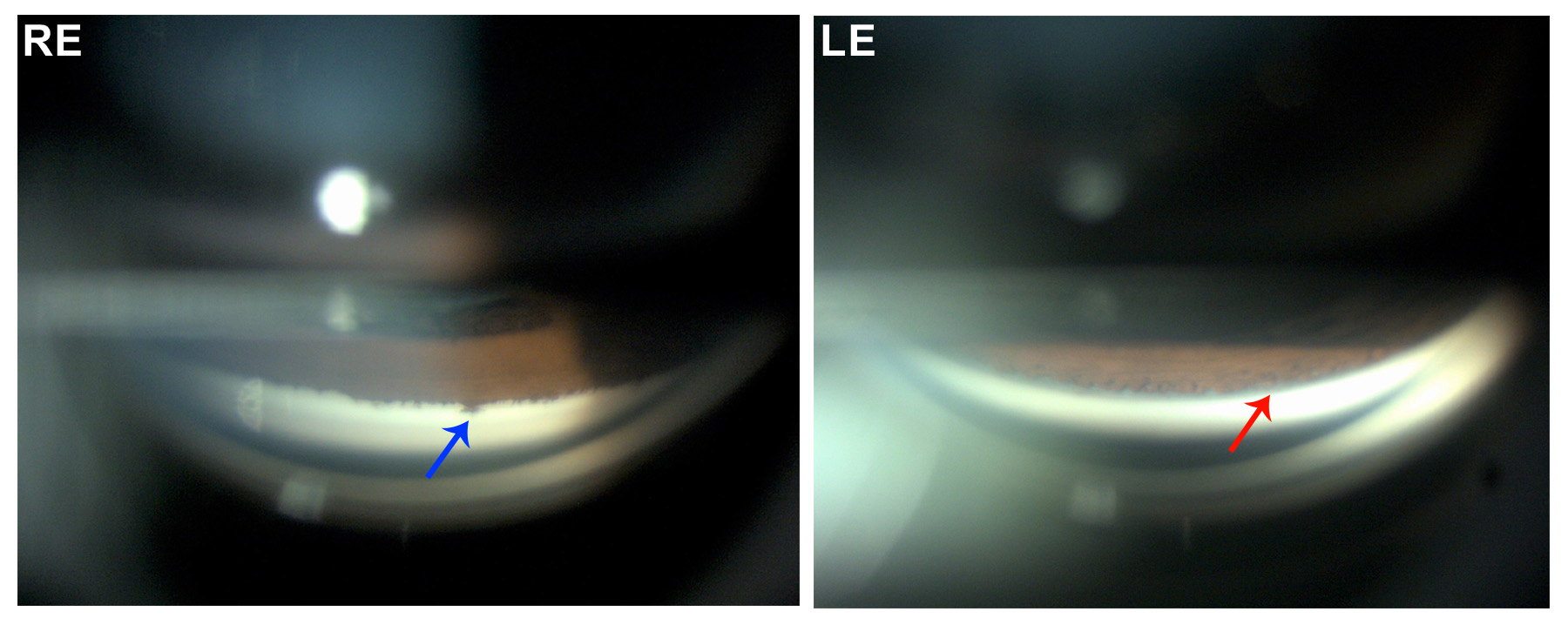
Figure 3. Fundus showing an advanced disc damage, note the central large pale area indicating enlarged cup (blue arrow), and a small cup in LE (red arrow).
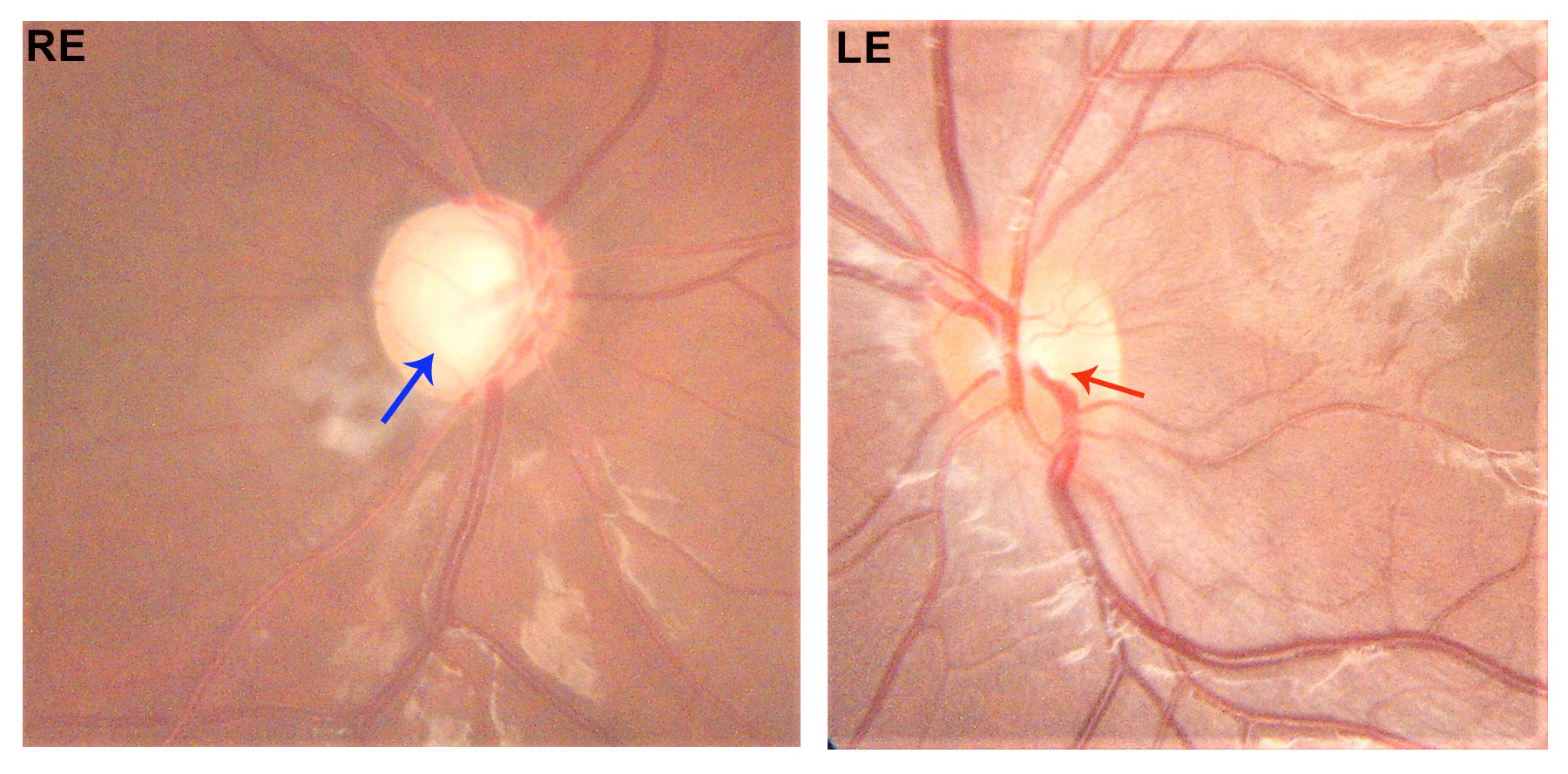
Figure 4. Slit lamp photography showing a filtering bleb in the right eye (blue arrow).
| | | | Discussion | Glaucoma in young age is relatively uncommon entity as compared to the elderly population and most often follows ocular comorbidities. The pupillary membrane is a remnant of a foetal membrane that persists as strands of tissue in the pupillary area. It exists as a source of blood supply to the lens in a foetus. It normally begins to regress in the sixth month and disappears completely by the eighth month of gestation.6 A failure of cellular activities that result in regression of pupillary membrane leads to PPM.7 PPM can be either unilateral or bilateral and can be variable in appearance, size, configuration and density.
In majority of the cases they appear as very thin fibres and are of no functional significance, patients usually remain asymptomatic. In rare cases, dense membranes can persist and obscure the pupil, causing amblyopia (lazy eye). Glaucoma associated with PPM is rare and has been reported sparsely in the past.8 Wagh et al reported a case of PPM with subacute angle closure (Partial closure of aqueous outflow pathway and sudden elevation of eye pressure causing eye pain and headache).3 But in that case the patient was a 36 year old female with bilateral PPM and her IOP and optic nerve head were normal. She was treated with Neodymium-doped Yttrium Aluminium Garnet (Nd: YAG) laser peripheral iridotomy (LPI) in BE. She had no glaucoma on presentation. Cibis et al reported a case series of 8 cases with anterior segment dysgenesis with secondary angle closure glaucoma.9 They classified the cases different from PPM as they had varying levels of anterior segment dysgenesis along with PPM. 3 patients underwent LPI along with pupilloplasty. The age of presentation was quite early in the series (within 1 year) and unilateral in presentation. In our case the presentation was at 11 years, the child and his family were not aware of the problem in his RE until recently. LPI was not considered in our case as the angles were open with intermittent pas. Earlier presentation and detection could have resulted in a better prognosis, preserving vision in our patient. Unlike in adults, glaucoma in children often fails to respond to medical management requiring early surgical intervention to prevent progression.10,11 In a study by Wiggs et al out of 23 juvenile glaucoma eyes 83% required glaucoma surgery for IOP control.12 Since the glaucoma in our case was in the advanced stage with very high IOP at presentation, early trabeculectomy was considered to safeguard the remaining vision in the affected eye.
| | | | Conclusion | | PPM can be easily identified with a simple torch light examination. Any child diagnosed/suspected with PPM must be referred for an ophthalmic evaluation as a close follow up is required in these children to prevent visual compromise due to possible amblyopia (lazy eye) and glaucoma. Early diagnosis will help in arresting the optic nerve damage and associated irreversible vision loss and help preserve quality of vision in these children. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Tasman W, Jaeger E. Duane's Ophthalmology. Philadelphia: Lippincott Williams & Wilkins; 2007. pp. 24-258.
- Chen CL, Peng J, Jia XG, Liu ZW, Zhao PQ. Hallermann-Streiff syndrome with bilateral microphthalmia, pupillary membranes and cataract absorption. Int J Ophthalmol. 2017;10(6):1016-1018. Published 2017 Jun 18. doi:10.18240/ijo.2017.06.30. [CrossRef]
- Wagh, Vijay & Venkatesh, Pradeep & Bhartiya, Prashant & Dada, Tanuj & Sethi, Harinder. (2005). Hyperplastic Persistent Pupillary Membrane Associated With Subacute Angle-Closure Glaucoma. Annals of Ophthalmology. 37. 51-53. 10.1385/AO:37:1:051. [CrossRef]
- Courtright, P., Hutchinson, A. K., & Lewallen, S. (2011). Visual impairment in children in middle- and lower-income countries. Archives of Disease in Childhood, 96(12), 1129-1134. [CrossRef] [PubMed]
- Senthil S, Badakere S, Ganesh J, Krishnamurthy R, Dikshit S, Choudhari N, Garudadri C, Mandal AK. Profile of childhood glaucoma at a tertiary center in South India. Indian J Ophthalmol. 2019 Mar;67(3):358-365. doi: 10.4103/ijo.IJO_786_18. PMID: 30777953; PMCID: PMC6407385. [CrossRef] [PubMed] [PMC free article]
- Goldberg MF. Persistent fetal vasculature (PVF): An integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous. Am J Ophthalmol. 1997;124:87-626. [CrossRef] [PubMed]
- Mandal AK, Netland PA. The Pediatric Glaucomas. Maryland Heights, MO: Elsevier, Butterworth Heinemann; 2006. p. 16.
- Johnson AT, Drack AV, Kwitek AE, Cannon RL, Stone EM, Alward WL. Clinical features and linkage analysis of a family with autosomal dominant juvenile glaucoma. Ophthalmology. 1993;100(4):524-529. [CrossRef] [PubMed]
- Cibis GW, Walton DS. Congenital pupillary-iris-lens membrane with goniodysgenesis J AAPOS. 2004;8:378-83. [CrossRef] [PubMed]
- Pathania D, Senthil S, Rao HL, Mandal AK, Garudadari CS. Outcomes of trabeculectomy in juvenile open angle glaucoma. Indian J Ophthalmol. 2014;62(2):224-228. [CrossRef] [PubMed] [PMC free article]
- Tsai JC, Chang HW, Kao CN, Lai IC, Teng MC. Trabeculectomy with mitomycin C versus trabeculectomy alone for juvenile primary open-angle glaucoma. Ophthalmologica. 2003;217(1):24-30. [CrossRef] [PubMed]
- Wiggs JL, Del Bono EA, Schuman JS, Hutchinson BT, Walton DS. Clinical features of five pedigrees genetically linked to the juvenile glaucoma locus on chromosome 1q21-q31. Ophthalmology. 1995;102(12):1782-1789 [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2025.3
|
| Cite this article as: | | R V C, S K, Venkatesh R, Shankar L G. Persistent Pupillary Membrane and Secondary Angle Closure Glaucoma: A Case Report. Pediatr Oncall J. 2025;22. doi: 10.7199/ped.oncall.2025.3 |
|