Amar Surjushe, Saurabh Jindal, Maithili Junagade, DG Saple.
Department of Dermatology, Venereology and Leprology, Grant Medical College and G T Hospital, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Amar Surjushe, Department of Dermatology,Venereology and Leprology,Grant Medical College and G. T. Hospital, Mumbai-400008.
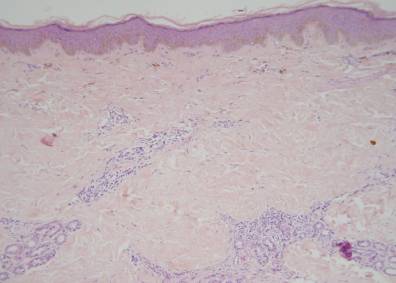
Email: dramarsurjushe@rediffmail.com | | Abstract | | Disabling pansclerotic morphoea of children is a rare, aggressive, and mutilating variant of deep morphea. It usually begins before the age of 14 years and has relentless progression and severe disability. In children, the localized form of scleroderma is more frequent than the systemic but both of them are rare, constituting less than 3% of rheumatic diseases in childhood. Approximately 1.5% of all scleroderma cases occur before 10 years of age (1, 2). We present a rare case of disabling pansclerotic morphea responded well to methotrexate. | | | | Keywords | | Disabling pansclerotic morphea, childhood, methotrexate | | | | Introduction | | Disabling pansclerotic morphea is a rare atrophying and sclerosing disorder that involves epidermis, dermis, subcutaneous tissue, muscle and bone (3). It begins with the extensor of extremities and progresses to involve the trunk, flexors, face, and scalp, sparing fingertips and toes. Diagnosis is based on the history, physical examination, and often skin biopsy. Though there are no specific therapies, various medications are used. Variable course of the disease with spontaneous remission in some cases and lack of standardization of outcome measures make evaluation of the effectiveness of these treatments challenging. We present a rare case of disabling pansclerotic morphea that was treated with methotrexate and responded well. | | | | Case Report | A 6-year old male child presented with tightness of skin of right leg since 1 year and difficulty in walking and straightening of right leg since 6 months. There was history of development of multiple hyperpigmented lesions over trunk, forearm, and face since 2 months. Cutaneous examination showed unilateral multiple hide bound hyperpigmented indurated plaques involving face, arm, forearm, abdomen, and lower limb of right side [Fig. 1A, 1B]. Investigation showed normal hemogram, liver, renal function tests; with ESR of 32 mm. Radiological survey was normal. Antinuclear antigen was positive in the titre of 1:40 while anti-double stranded DNA; anti-scleroderma antibodies (anti-Scl 70) were negative. Skin biopsy from indurated plaque showed atrophic epidermis and thickened dermis with dense collagen [Fig. 2]. Patient was started on weekly methotrexate in the dose of 5 mg/m²/week (7.5mg/week) with monitoring of hematological, liver and renal parameters. After 10 cycles there were no new lesions and no increase in the old lesions and few lesions showed decreased induration. At present, patient has completed 20 cycles of the pulse.
Figure: 1 A Hyperpigmented depressed plaque present on right side of the face.

Figure: 1 B Hyperpigmented depressed plaque on right thigh and lower limb.

Fig.2- Skin biopsy showing thickened dermis with dense collagen
 | | | | Discussion | Disabling pansclerotic morphea is a variant of localized scleroderma characterized by a rapid progression of cutaneous fibrosis with extension to joints and fascia. Various modalities of treatment are mentioned in the literature but with little effect. The response is often poor and in most patients the condition is progressive (4) and occasionally fatal (3). High dose of parenteral penicillin or ceftriaxone along with oral corticosteroid given in several courses over a time span of several months has beneficial effect in early cases (5). Phototherapy with UVA-1 (340-400 nm) has been found to be effective because of induction of interstitial collagenase [matrix metalloproteinase-1 (MMP-1)] and immunomodulation through induction of cytokines (6). Other therapeutic modalities tried with varying results are calcitriol (7), D-penicillamine (8), cyclosporine (9), and topical calcipotriene (10). Several therapies that may hold promise are thalidomide and newer anti-tumor necrosis factor treatments (etanercept, infliximab).
Low dose methotrexate had also being tried in widespread morphea (11, 12, 13). It inhibits dihydrofolic acid reductase enzymes involved in the synthesis of ribonucleic and deoxyribonucleic acids. The exact mechanism of action in localized scleroderma has not been well evaluated (11). Uziel et al. used methotrexate along with methyl prednisolone pulse (14). Combination of MTX and pulse methyl prednisolone is well tolerated and appears to be effective in the treatment of localized scleroderma. In our case response to methotrexate suggests its efficacy in reducing skin induration although further studies are needed. Surgical treatment like bone grafting, tissue expansion and microsurgical reconstruction may be required in cases of progressive facial hemiatrophy (15). | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Black CM: Prognosis and management of scleroderma and scleroderma-like disorders in children. Clin Exp Rheumatol 1994; 12:75-81.
- Vancheeswaran R, Black CM, David J, et al: Childhood-Onset Scleroderma: Is it different from Adult-Onset Disease- Arthritis Rheum 1996; 39:1041-1049. [CrossRef] [PubMed]
- Diaz Perez JL, Connolly SM, Winkelmann RK. Disabling pansclerotic morphoea of children. Arch Dermatol 1980; 16:169-73. [CrossRef]
- Wollina U, Wollina K. Pansclerotic Morphoea of childhood: follow up over 6 years. Paediatr Dermatol 1999; 16: 245-7. [CrossRef]
- Fitzpatrick Color atlas and synopsis of Clinical Dermatology - Common and serious diseases. Fitzpatrick TB, Johnson RA, Wolff K, Suurmond D. 4th Ed. 2001.
- Scharffetter - Kochanek K, Goldermann R, Lehmann P, Holzle E, Goerz G. PUVA therapy in disabling pansclerotic morphoea of children. Br J Dermatol 1995; 132:830-1. [CrossRef] [PubMed]
- Hulshof MM, Pavel S, Breedveld FC, et al: Oral calcitriol as a new therapeutic modality for generalized morphea. Arch Dermatol 1994; 130:1290-1293. [CrossRef] [PubMed]
- Falanga V, Medsger TA: D-penicillamine in the treatment of localized scleroderma. Arch Dermatol 1990; 126:609-612. [CrossRef] [PubMed]
- Peter RU, Rizicka T, Eckert F. Low dose ciclosporin A in the treatment of disabling morphoea. Arch Dermatol 1991; 127:1420-21. [CrossRef] [PubMed]
- Cunningham BB; Landells IDR, Langman C, et al: Topical calcipotriene for morphea/linear scleroderma. J Am Acad Dermatol 1998; 39:211-215. [CrossRef]
- Seyger MMB, Van Den Hoogen FHJ, De Boo T, De Jong EMGJ. Low dose methotrexate in the treatment of widespread morphoea. J Am Acad Dermatol 1998; 39:220-5. [CrossRef]
- Seyger MM, Van Den Hoogen FH, Van Vlijem Willems IM, Van De Kerkhof PC, De Jong EM. Localised and systemic scleroderma shows different histological responses to methotrexate therapy. J Pathol 2001; 193:511-6. [CrossRef]
- Kreuter A, et al. Pulsed high dose corticosteroids combined with low dose Methotrexate in severe localized Scleroderma. Arch Dermatol 2005; 141:847. [CrossRef] [PubMed]
- Uziel Y, Feldman BM, Krafchik BR, Yeung RS, Laxer RM: Methotrexate and corticosteroid therapy for pediatric localized scleroderma. J Pediatr 2000; 136: 91-95. [CrossRef]
- Sehgal VN, Srivastava G, Aggarwal A, Behl PN, Choudary M, Bajaj P. Localised Scleroderma / Morphea. Int J Dermatol 2002;41:467-75. [CrossRef] [PubMed]
|
| Cite this article as: | | Surjushe A, Jindal S, Junagade M, Saple D. Disabling Pansclerotic Morphoea of Children Treated with Methotrexate. Pediatr Oncall J. 2007;4: 12-13. |
|