Novina Novina1, Annang Giri Moelyo2, Erni Nuraeni1, Maria Lisa Mihardja3, Yanuar Ariefudin4, Faisal Faisal1, Aman B Pulungan5.
1Endocrinology Division, Department of Child Health, Faculty of Medicine, Universitas Padjadjaran, Hasan Sadikin General Hospital, Bandung, West Java Indonesia,
2Endocrinology Division, Department of Child Health, Faculty of Medicine, Universitas Sebelas Maret, Dr. Moewardi General Hospital, Solo, Central Java Indonesia,
3Pediatric Resident Department of Child Health, Faculty of Medicine Universitas Padjadjaran, Bandung, West Java Indonesia,
4Pediatric Resident Department of Child Health, Faculty of Medicine, Universitas Sebelas Maret, Solo, Central Java Indonesia,
5Department of Child Health, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
ADDRESS FOR CORRESPONDENCE
Novina, Department of Child Health, Faculty of Medicine, Universitas Padjadjaran/Hasan Sadikin General Hospital, Bandung, West Java Indonesia.
Email: novina@unpad.ac.id. | | Abstract | Objective: The aim of this study is to describe the impact of the COVID-19 pandemic on Glycemic Control (GC) in children with Type 1 Diabetes Mellitus (T1DM) and the role of online consultation.
Methods: We conducted a cross-sectional analytical study of children with T1DM who were controlled at Pediatric Endocrinology Clinic Hasan Sadikin General Hospital (RSHS) and Dr. Moewardi General Hospital (RSDM) before and during the COVID-19 pandemic. We compare average HbA1c levels before and during the COVID-19 era for the GC parameter.
Results: A total of 55 children with T1DM were recruited in this study: 29 boys [52.7%] and 26 girls [47.3%]; the majority are adolescents [74.5%], mean age: 13.47 ± 3.1 years, the median duration of suffering from diabetes: 33 months. We did a paired t-test on 50 children with the result that average HbA1c significantly decrease from 10.3± 2.3% to 9,4±2.0 % before and during the pandemic era (p<0.001). There was a significant increase in BMI (0.75, p=0.001) but do not significantly correlate with HbA1c values before and during the pandemic.
Conclusion: There has been a significant decrease in HbA1c during the COVID-19 pandemic. Implementation of work-from-home and semi-lockdown policy encourages parents to monitor the GC of their children better. Pediatric endocrinologists and residents in RSHS and RSDM assisted patients and their parents in achieving better GC during the COVID-19 pandemic through proper consultation, education and medical escort for outpatient clinics and online consultations using a social media group specially designated for T1DM families.
| | | | Keywords | | type 1 diabetes mellitus, glycemic control, HbA1c, BMI, COVID-19, online consultation. | | | | Background | The prevalence of type 1 diabetes mellitus (T1DM) as the most common chronic endocrine disorder in children has risen significantly over the last decade. Type 1 diabetes mellitus is caused by the progressive destruction of pancreatic beta cells, leading to an absolute deficiency of insulin secretion that subsequently proceeds into a hyperglycemic state.1,2 Maintenance of good glycemic control (GC) can prevent the progression of the disease into acute complications such as episodes of hypoglycemia and diabetic ketoacidosis (DKA) and chronic complications such as neuropathy, nephropathy, retinopathy and cardiovascular problems. The recommendation parameter for assessing GC by diabetes organization is quarterly hemoglobin A1C (HbA1c) with the target <7% for children and adolescents. Regular intensive insulin regimens, frequent glucose monitoring, caloric and carbohydrate intake measurement, appropriate physical activity and prompt consultation with a doctor are ways to maintain GC in children. Parents, caregivers and doctors' involvement are essential for satisfactory GC in children with T1DM.3,4
Coronavirus disease 2019 (COVID-19) has severely impacted all countries and was declared a global pandemic on 11 March 2020.5 The concerns were raised for patients with chronic disorders like diabetes. Government policies like regional quarantines, restrictions on outdoor activities, postponing school activities and mandatory staying at home may affect GC children with T1DM. Rigid restrictions on outdoor activities and mandatory staying at home may reduce attendance to the health care facility and also limit consultation with the doctor.6 From the global survey, it was stated that limited contact with diabetes or endocrine teams in the majority of centers, mostly due to fear of COVID-19 by families. The other problem was a need for more supplies for managing DM, such as glucose test strips, basal and bolus insulins. The last, social distancing practices shifted daily routine into a sedentary lifestyle. These problems might have a negative impact on long-term GC during the pandemic.7,8
Conversely, few studies showed an improvement in GC in children with T1DM during the lockdown. It is associated with more organized insulin administration timing and limited nutrition intake. Parents or caregivers also have more attention to controlling the GC of their children.9
Another issue was reciprocal association between COVID-19 and DM. A global survey in 51 pediatrics centers showed more moderate to severe symptoms in DM children with confirmed COVID-19, of which 15.9% needed non-invasive ventilation and 9.7% intubated. Conversely, family fears of COVID-19 pandemic could delay hospital admission for emergency cases in T1DM children, resulting in a higher proportion of DKA.8
Implementing telemedicine health services is an alternative way for coping with difficulties to do on-site consultations with the doctors in the hospital. Telemedicine is a powerful tool that allows the continuity of healthcare services while minimizing the spread of COVID-19. One study in Egypt used simple basic ways of telemedicine service in managing T1DM through sharing data from logbooks and adjusting insulin regimens. From that research, 70% of patients and their families feel satisfied.10 In Hasan Sadikin General Hospital (RSHS) and Dr. Moewardi General Hospital (RSDM), we still need to implement telemedicine, but we both do have active social media groups specially designated for T1DM families. Pediatric endocrinologists and residents always educate and give online consultations through that group regularly. Also, we do phone consultations if some T1DM cases need further explanation. It is important for children and their families with T1DM to strive for sufficient GC and still get proper consultation from healthcare providers, even in the COVID-19 pandemic situation.
| | | | Methods | This study is a cross-sectional study approved by the ethical committee of RSHS and RSDM. The participant was children and adolescent (1-<18 years) with T1DM who enrolled in a pediatric endocrinology clinic. Inclusion criteria measured HbA1c minimal three times and used the same insulin regimen therapy (multiple daily injections), while exclusion criteria had other chronic diseases.
We collected data in RSHS (West Java) and RSDM (Central Java) from medical records with time points before the pandemic from November 1st, 2018, to February 28th, 2020 and during the pandemic COVID-19 March 1st, 2020 until June 30th, 2021 (16 months vs 16 months).
Individual characteristics such as age, sex, duration of diabetes, body weight and height were collected from the registry and medical records. Age was divided into three groups based on the Indonesian Ministry of Health 0-4 years (under 5 years old), 5-11 years (childhood) and 12-18 years (adolescent). Weight and height were measured to calculate body mass index (BMI). Weight was recorded to the nearest 0.1 kg using an electronic weighing scale. Height was measured using a microtoise stadiometer to the nearest millimeter. The child must stand back to the wall with head in Frankfort horizontal position, heels at the wall, ankles together and knees and spine straight against a vertical metal rule permanently attached to the wall or a wide upright board. Height is measured at the top of the head by a sliding perpendicular plate. Body mass index was plotted into BMI-for-age percentile based on the CDC growth charts for children and teens (ages 2 through 19 years). Body mass index was categorized into underweight (< 5th percentile), normal ( >5th and < 85th percentile), overweight ( >85th dan < 95th), obesity ( > 95th percentile). We compare average HbA1c (minimum criteria had 3 HbA1c values at least) and BMI before and during the COVID-19 pandemic.
Data are presented descriptively and analytically. Descriptive analysis shows statistical measures in the form of numbers for categorical data. Data processing was analyzed using Statistical Package for the Social Sciences (SPSS) 20 software program (SPSS, Chicago, IL, USA). Comparison of HbA1c values and BMI before and during the COVID-19 era were analyzed with paired t-tests. The significance of the test results was determined based on p <0.05.
| | | | Results | This study enrolled 55 patients with a mean age of 13.47 ± 3.1, a median age of 14 years and a range from 5 to 17 years. The majority of patients were in adolescent age (74.5%), both in West (79.5%) and Central Java (62.5%). Twenty-nine (52.7%) patients were boys and 26 (47.3%) were girls. The mean and median BMI pre-post pandemic consecutively was 18.78 ± 4.56, 19.33 ± 4.44, 18.1 and 18.9 kg/m2. Only a minority had an abnormal baseline BMI before the pandemic (17.6% underweight, 7.9% overweight and 3.9% obese). The median duration of T1DM is 33 months, with an interquartile range of 16-54 months.
All participants were on multiple daily injections of insulin regimens and were on national health insurance called BPJS Kesehatan (health care and social security agency). The majority of parents educational status are senior high school graduates. Some patients come from a low socioeconomic status family (40.5%) with a median income three million Indonesian Rupiah (IDR).
Descriptive data comprised of patients’ characteristics are described in Table 1.
Table 1. Subject characteristics (n=55).
| Characteristics |
All Samples
(n=55) |
Location |
p-value |
West Java
n=39 (70.9%) |
Central Java
n=16 (29.1%) |
| Age (years) |
|
|
|
|
| Median (IQR) |
14 (11-17) |
15 (12-17) |
13 (10-15) |
0.036 |
| Age (years) |
|
|
|
|
| 0-4 |
0 (0%) |
0 (0%) |
0 (0%) |
|
| 5-11 |
14 (25.5%) |
8 (20.5%) |
6 (37.5%) |
0.306 |
| 12-18 |
41 (74.5%) |
31 (79.5%) |
10 (62.5%) |
|
| Gender |
|
|
|
|
| Male |
29 (52.7%) |
24 (61.5%) |
5 (31.3%) |
0.041 |
| Female |
26 (47.3%) |
15 (38.5%) |
11 (68.7%) |
|
| Duration of T1DM (months) |
|
|
|
|
| Median (IQR) |
33 (16-54) |
37 (24-66) |
18 (7-43) |
0.022 |
| Body Mass Index (kg/m2) |
n=51 |
n=35 |
n=16 |
|
| Median (IQR) |
18.1 (15.9-21.5) |
18.3 (16.0-21.7) |
18.0 (14.6-19.7) |
0.465 |
| Body Mass Index for Age |
n=51 |
n=35 |
n=16 |
|
| Underweight |
9 (17.6%) |
6 (17.1%) |
3 (18.8%) |
0.784 |
| Normal |
36 (70.6%) |
24 (68.6%) |
12 (75.0%) |
|
| Overweight |
4 (7.9%) |
3 (8.6%) |
1 (6.2%) |
|
| Obese |
2 (3.9%) |
2 (5.7%) |
0 (0.0%) |
|
| Mother’s Education |
n=42 |
n=26 |
n=16 |
|
| Elementary School |
4 (9.6%) |
3 (11.5%) |
1 (6.2%) |
|
| Junior High School |
3 (7.1%) |
1 (3.8%) |
2 (12.5%) |
|
| Senior High School |
27 (64.3%) |
16 (61.5%) |
11 (68.8%) |
|
| University Graduate |
8 (19.0%) |
6 (23.1%) |
2 (12.5%) |
|
| Father’s Education |
n=42 |
n=26 |
n=16 |
|
| Elementary School |
3 (7.1%) |
2 (7.7%) |
1 (6.3%) |
|
| Junior High School |
7 (16.7%) |
6 (23.1%) |
1 (6.3%) |
|
| Senior High School |
23 (54.8%) |
10 (38.5%) |
13 (81.1%) |
|
| University Graduate |
9 (21.4%) |
8 (30.8%) |
1 (6.3%) |
|
| Family Income (in million IDR) |
n=26 |
n=26 |
n=16 |
|
| Median (IQR) |
3 (2-5) |
3 (2-5) |
4 (4-4) |
|
Characteristics are presented as mean ± standard deviation, median (interquartile range), or frequency (%)
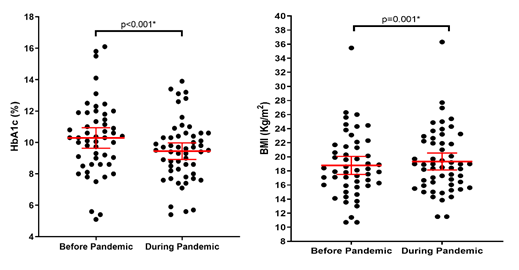
There is a significant decrease in HbA1c prior and during the COVID-19 era. We do have 50 completed data of HbA1c. From paired t-test of 50 children, there was a significant decrease in average HbA1c from 10.34 ±2.33% to 9.4±2.01 % (0.94, p<0.001). Body mass index also showed significant increase of about 0.75 (18.78±4.56 to 19.53±4.53, p 0.001).
Table 2. HbA1c of Children with Type 1 Diabetes Mellitus Prior and During COVID-19 Era.
| Variable |
Before Pandemic |
During Pandemic |
Mean of Difference (95% CI) |
p-value |
| HbA1c (%) |
n=50 |
n=50 |
|
|
| Mean±SD |
10.34 ± 2.33 |
9.40 ± 2.01 |
0.94 (0.53-1.34) |
<0.001* |
| BMI (kg/m2) |
|
|
|
|
| Mean±SD |
18.78 ± 4.56 |
19.53 ± 4.53 |
-0.75 (-0.33 – (-1.17)) |
0.001* |
Figure 1. Difference between HbA1c levels and BMI by Scatter Plots.
The female group has more decrease in HbA1c than boys’ group (1.02 vs 0.86). Both groups significantly decreased HbA1c (10.58% to 9.72% in the boys’ group, p=0.004 and 10.07% to 9.05% in the girls’ group, p=0.005). The children group has greater decrease in HbA1c value than the adolescent group. (1.18% vs 0.86%), but both groups significantly decreased HbA1c (9.7% to 8.53% in the children group, p=0.046 and 10.54% to 9.67% in the adolescent group, p < 0.001). There were equally no significant differences in A1C between boys‘ vs girls’ groups (p=0.695) and children vs adolescent groups (p=0.517). There was no significant correlation between the change in BMI and HbA1c levels before-during the COVID-19 pandemic. (p=0.487 before pandemic, p=0.435 during pandemic). The data is presented in Tables 3 and 4.
Table 3. HbA1c of Children with Type 1 Diabetes Mellitus Before and During the COVID-19 Era by patient characteristic.
| Variable |
n |
HbA1c Before Pandemic n=50 |
HbA1c During Pandemic n=50 |
Change in HbA1c before to during pandemic |
p-value (within) |
p-value (between) |
| Mean (%) ±SD |
Mean (%) ±SD |
Mean of Difference (95% CI) |
| Sex |
|
|
|
|
|
|
| Male |
26 |
10.58 ± 2.45 |
9.72 ± 1.94 |
0.86 (0.31-1.42) |
0.004* |
0.695 |
| Female |
24 |
10.07 ± 2.22 |
9.05 ± 2.07 |
1.02 (0.39 – 1.66) |
0.005* |
|
| Age |
|
|
|
|
|
|
| 0-11 years |
12 |
9.70 ± 2.16 |
8.53 ± 1.66 |
1.18 (0.03 – 2.32) |
0.046* |
0.517 |
| 12-18 years |
38 |
10.54 ± 2.38 |
9.67 ± 2.05 |
0.86 (0.44 – 1.29) |
<0.001* |
|
Table 4. Change of BMI Against HbA1c Before and During Pandemic.
| Variable |
HbA1c Before Pandemic |
HbA1c During Pandemic |
Change in HbA1c before to during pandemic |
| r |
p |
r |
p |
r |
p |
| Change in BMI |
-0.005 |
0.487 |
0.024 |
0.435 |
-0.022 |
0.440 |
| | | | Discussion | This study reports a significant reduction of HbA1c compared to before and during COVID-19, although still less than the optimal target. A significant decrease in HbA1c occurred in both children (p=0,46) and adolescents (p=0,001). Better improvement of GC was shown in the children group (1- < 11 years) than in adolescent with a greater decrease of HbA1c (1.18 vs 0.86), even though the comparison are not significant (p=0.517).
Based on previous research, the teenage population has more difficulties achieving targeted GC. Many factors are concerned, including physiological changes leading to greater insulin resistance during puberty, shifting responsibility for managing T1DM from parents to teens, social peer pressure and psychological and emotional problems related to chronic illness fatigue.11 Influence of the family environment for GC may be less relevant in teenagers due to the desire for detachment, independence and autonomy in the adolescent phase, differently from children.12
A study in Italia displayed that children and adolescents with T1DM have had significant positive effects in decreasing HbA1c related to COVID-19 lockdown, caused by more regularity in the management of insulin therapy and more careful control of glycemic values by the patients and parents/caregivers, leading into better long-term GC.8 Previous study in Egypt shown different results that HbA1c did not change significantly in toddlers and preschoolers (8.55 ± 1.33 to 8.08 ± 1.22, p=0.28) before and after lockdown, meanwhile children (8.6 ± 1.2 to 8.94 ± 1.64, p=0.001) and adolescents (8.65 + 1.27 to 9.28 ± 2.01, p=0.003) had significant worsening during COVID-19 pandemic. The increase in HbA1c occurred due to limited outdoor activities and the increased desire for snacks, especially when doing virtual learning.10 The contradictive result was shown from a study in Italy by Elina H et al. It was stated that the adolescent group (12-15.9 years) improved their GC significantly. The speculative reason was that teenagers spend their time mostly at home instead of leisure time with friends outside.13
The decrease in HbA1c in males and females differed significantly before and during the pandemic. Females were decreased greater than the males (1.02 vs. 0.86), but there were no significant differences between both groups (p=0.695). This was inconsistent with another report by Setoodeh et al., that females have less sensitivity to insulin and a risk factor for poorer GC.14
To overcome the COVID-19 pandemic situation, the government limited people’s daily activities by applying some policies such as implementing working from home, transitioning schools into virtual modes of education, closing most public places for leisure and restriction for travelling to different cities or countries.15 Parents who stayed at home had more time to manage the GC of their T1DM children. Full-time parents could probably balance diet, schedule meals and monitor insulin injections, which might be difficult when children have school activities.12 Study conducted in Italy in T1DM pre-school and school children (mean age 8,7 ± 1,9 years) explained better GC marked by a higher median value of time in range (TIR) and lower mean values of time above range (TAR) from CGM records during COVID-19 period. The better results might be associated with the return of parental care due to stay-at-home regulations. Schedule meals at home by parents than meals outside, such as in the school canteen or restaurants with friends, can make more accurate carbohydrate counting and contribute to satisfactory GC.16
Children mostly at home during the COVID-19 pandemic without any outdoor physical activities (PA) could have a negative effect on GC. Physical activity, insulin and diet are components of blood glucose regulation. Glycemic control of Italian T1DM adolescents (median age 14.2 years) improved in groups who exercised regularly during the COVID-19 pandemic and surprisingly did not worsen in those who did not exercise. The counter reason attributed to this result could be continuous monitoring from parents more closely than usual in the pandemic situation.17,18 Restriction of the COVID-19 pandemic does not mean all types of physical activity must be stopped. Simple and easy PA at home (indoor jogging, skipping rope, or online classes) can be an alternative way to apply exercise while still maintaining social distancing.19 From phone consultation with parents in our study, we have got information that some children still do indoor jogging or play football in the home yard during the pandemic.
There was a significant increase in BMI in our study (from 18.78 ± 4.56 to 19.53 ± 4.53, p<0.001). COVID-19 pandemic has changed the lifestyle of children and adolescents into sedentary and less PA. A significant increase in BMI and body weight during lockdown was found in research in 150 Saudi Arabian children and adolescents with T1DM. Most patients reported a decrease in PA and frequent unhealthier consumption during the lockdown, which predisposed them to difficulties in GC.20 This present study shows the opposite outcome, which there is an increase in BMI along with an improvement of HbA1c, although changes in BMI do not statistically significant correlate with HbA1c before and during the pandemic (r=-0.022, p=0.44). The plausible reason that explains the results is the catabolic state driven by insulin deficiency in patients with T1DM. insulin is one of the anabolic hormones that promote lipogenesis and inhibit protein catabolism. insulin therapy can conserve ingested calories; it concluded that weight gain during insulin therapy might be associated with improved GC and lower weight may indicate inadequate insulin treatment. Analysis of an observational study in T1DM Korean adults found an inverse relationship between BMI and HbA1c levels in the low BMI group. At the same time, a positive correlation was seen in the high BMI group.21 Reported detrimental consequences of excessive weight gain include increased blood pressure and dyslipidemia, which increase cardiovascular risk complications later in T1DM patients.22 Majority of subjects in this study had normal BMI before and during the COVID-19 pandemic. Change in BMI was seen in 6 subjects (underweight to normal [6%], normal to overweight [4%] and obese to overweight [2%]) and there was no excessive weight gain (less than 20% in 2 subjects with normal BMI group before pandemic).
There are many contradictive results about the GC of children with T1DM during the pandemic era. Studies with larger samples in South Alabama showed decreased HbA1c (9.2 to 9.5%) during the quarantine COVID-19 period. In that research, patients with public health insurance had significantly higher HbA1c before and during the quarantine phase.6 All participants in our study were on national health care insurance, so it did not influence the research results. Other factors that may be contributed to GC were socioeconomic status and parents’ education.22 Poor compliance, mainly due to the cost of insulin and glucose strips, is one of the main factors for sub-optimal GC in developing countries. Additionally, during the COVID-19 pandemic, lack of medical supplies, medication and medical care could not be avoided, further impacting the GC of T1DM people. Verma et al. demonstrated that the nonavailability of glucose strips or insulin would have a negative effect on the GC of T1DM samples (mean age 11.9 years) in India.23 Another study in India showed different perspectives that children from lower and middle socio-economic classes showed a better GC post-lockdown. In contrast, GC’s children from higher socio-economic class had unchanged. In that cohort study, the provision of free insulin, especially to lower-income families, could be one reason for improved GC.24 Some subjects in our study come from low socioeconomic families (40.5%) and most parents are senior high school graduates. At the beginning of the pandemic, to prevent COVID-19 transmission, parents were allowed not to bring their children to the hospital. They could get insulin supplies with dosage as needed based on children’s blood glucose daily records. Although face-to-face consultations are restricted, parents could still get insulin dosage adjustments done through online consultations with pediatric endocrinologists or residents via social media groups or phones. Sometimes parents in that social media group also exchange information actively about the availability of insulin during the pandemic or share if there are excess supplies among them.
Telemedicine is the way to pursue better GC while maintaining social distancing and minimizing the SARS-CoV-2 transmission. Research in Italia showed that usage of telemedicine during lockdown improved GC based on ambulatory glucose profile data in children and adolescents with T1DM.25 In our study, we still need to implement telemedicine, but parents still get proper consultation and education actively via social media groups specially designated for T1DM families. Pediatric endocrinologists and residents routinely communicate and monitor T1DM parents and children via that group. These methods were alternative ways while telemedicine still could not use yet in unexpected pandemic situations. In our study, routine consultation and monitoring from medical staff might be considered factors contributing to decreased HbA1c levels.
Managing T1DM children during the pandemic situation is very challenging. It is already known that COVID-19 infection is associated with worsening diabetes symptoms and vice versa. An additional issue was added based on retrospective cohort studies by the Centers for Disease Control and Prevention (CDC). That report proved that the pediatric population (less than 18 years) was more likely to be diagnosed as newly DM more than 30 days after infection than those without COVID-19. Consequently, pediatricians and pediatric endocrinologists must be prepared for the possibility of increasing DM cases in children during the pandemic. Two-way negative relations between DM and COVID-19 must always be considered when handling T1DM children in these situations.26
There were a few limitations in our study. Firstly, the assessment of GC was only based on HbA1c and did not include home blood glucose documentation by finger pricks. The other limitation was no specific data about our patients' physical activities and carbohydrate consumption. However, our study combined two tertiary hospitals in Java Island, Indonesia and depicted innovative ways of caring for children with T1DM during the pandemic. In conclusion, a positive impact of GC during the COVID-19 pandemic was seen in children and adolescents with T1DM. It is emphasized that collaboration between healthcare professionals and parents is the primary key to maintaining good GC during the unusual pandemic situation, even in developing countries.
| | | | Conclusion | | There has been a significant decrease in HbA1c in T1DM children in West and Central Java, Indonesia during the COVID-19 pandemic. Implementing work-from-home and semi-lockdown policies encourages parents to monitor GC better and limit their children's glucose consumption. This study's significant increase in BMI results from weight gain that commonly happens in insulin treatment. Pediatric endocrinologists and residents in RSHS and RSDM assisted patients and their parents in achieving better GC during the COVID-19 pandemic through proper consultation, education and medical escort for outpatient clinics and online consultations using a social media group specially designated for T1DM families. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Pulungan AB, Fadiana G, Annisa D. Type 1 diabetes mellitus in children: experience in Indonesia. Clinical Pediatric Endocrinology. 2021;30(1):11-8. [CrossRef] [PubMed] [PMC free article]
- Mayer-Davis EJ, Kahkoska AR, Jefferies C, Dabelea D, Balde N, Gong CX, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatric Diabetes. 2018;27(27):7-19. [CrossRef] [PubMed] [PMC free article]
- DiMeglio LA, Acerini CL, Codner E, Craig ME, Hofer SE, Pillay K, Maahs DM. ISPAD Clinical Practice Consensus Guidelines 2018: Glycemic control targets and glucose monitoring for children, adolescents, and young adults with diabetes. Pediatric Diabetes. 2018;27:105-4. [CrossRef] [PubMed]
- American Diabetes Association. Children and Adolescents: Standards of Medical Care in Diabetes-2020. Diabetes Care.2020;43(1):163-82. [CrossRef] [PubMed]
- World Health Organization. Coronavirus disease 2019 (COVID19): situation report 65. March 2020.https://www.who.int/docs/defaultsource/coronaviruse/situation-reports/20200325-sitrep-65- covid-19.pdf.
- Gayoso M, Lim WY, Mulekar MS, Kaulfers AD. Effect of Covid-19 quarantine on diabetes Care in Children. Clinical Diabetes Endocrinology. 2021;7(1):9. doi: 10.1186/s40842-021-00122-x. [CrossRef] [PubMed] [PMC free article]
- Elbarbary NS, dos Santos TJ, de Beaufort C, Wiltshire E, Pulungan A, Scaramuzza AE. The Challenges of Managing Pediatric Diabetes and Other Endocrine Disorders During the COVID-19 Pandemic:Results From an International Cross-Sectional Survey. Frontiers in Endocrinology. 2021;12:735554. doi: 10.3389/fendo.2021.735554. [CrossRef] [PubMed] [PMC free article]
- Marigliano M, Maffeis C. Glycemic control of children and adolescents with type 1 diabetes improved after COVID-19 lockdown in Italy. Acta Diabetologica. 2021 ;58(5):661-4. doi: 10.1007/s00592-020-01667-6. [CrossRef] [PubMed] [PMC free article]
- Wu X, Luo S, Zheng X, Ding Y, Wang S, Ling P, et al. Glycemic control in children and teenagers with type 1 diabetes around lockdown for COVID-19: A continuous glucose monitoring-based observational study. Journal of Diabetes Investigation. 2021;12(9):1708-17. [CrossRef] [PubMed] [PMC free article]
- Elhenawy YI, Eltonbary KY. Glycemic control among children and adolescents with type 1 diabetes during COVID-19 pandemic in Egypt: a pilot study. International Journal of Diabetes in Developing Countries. 2021;41: 389-95. [CrossRef] [PubMed] [PMC free article]
- Unnikrishnan R Shah VN, Mohan, V. Challenges in diagnosis and management of diabetes in the young. Clinical Diabetes and Endocrinology.2016;2(18). https://doi.org/10.1186/s40842-016-0036-6 [CrossRef] [PubMed] [PMC free article]
- Di Dalmazi G, Maltoni G, Bongiorno C, Tucci L, Natale VD, Moscatiello S, et al. Comparison of the Effects of Lockdown due to COVID-19 on Glucose Patterns Among Children, Adolescents, and Adults with Type 1 Diabetes: CGM Study. BMJ Open Diabetes Research and Care.2020;8(2). doi:10.1136/ bmjdrc-2020-001664. [CrossRef] [PubMed] [PMC free article]
- Hakonen E, Varimo T, Tuomaala AK, Miettinen PJ, Pulkkinen MA. The Effect of COVID-19 Lockdown on the Glycemic Control of Children with Type 1 Diabetes. BMC Pediatrics .2022;22(48):1-8. [CrossRef] [PubMed] [PMC free article]
- Cheng HP, Wong JSL, Selveindran NM, Hong JYH. Impact of COVID-19 Lockdown on Glycemic Control and Lifestyle Changes in Children and Adolescents with Type 1 and Type 2 Diabetes Mellitus. Endocrine. 2021 ;73(3):499-506. [CrossRef] [PubMed] [PMC free article]
- Choudhary A, Adhikari S, White PC. Impact of the COVID-19 Pandemic on Management of Children and Adolescents with Type 1 Diabetes. BMC Pediatric.2022; 22(124).https://doi.org/10.1186/s12887-022-03189-2. [CrossRef] [PubMed] [PMC free article]
- Schiaffini R, Barbetti F, Rapini N, et al. School and pre-school children with type 1 diabetes during Covid-19 quarantine: The synergic effect of parental care and technology. Diabetes Research and Clinical Practice. 2020;166:108302. doi:10.1016/j.diabres.2020.108302 [CrossRef] [PubMed] [PMC free article]
- Tornese G, Ceconi V, Monasta L, Carletti C, Faleschini E, Barbi E. Glycemic Control in Type 1 Diabetes Mellitus During COVID-19 Quarantine and the Role of In-Home Physical Activity. Diabetes Technology and Therapeutics. 2020;22(6):462-7. [CrossRef] [PubMed]
- Turan H, Güneş Kaya D, Tarçın G, Evliyaoğlu SO. Effect of the COVID-19 Quarantine on Metabolic Control in Children and Adolescents with Type 1 Diabetes. Endocrinología, Diabetes y Nutrición (English edition). 2021;69(3):201-8. [CrossRef] [PubMed] [PMC free article]
- Bentlage E, Ammar A, How D, Ahmed M, Trabelsi K, Chtourou H, et al. Practical Recommendations for Maintaining Active Lifestyle During the COVID-19 Pandemic: A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2020;17:6265. http://dx.doi.org/10.3390/ijerph17176265. [CrossRef] [PubMed] [PMC free article]
- Al Agha AE, Alharbi RS, Almohammadi OA, Yousef SY, Sulimani AE, Alaama RA. Impact of COVID-19 Lockdown on Glycemic Control in Children and Adolescents. Saudi Medical Journal. 2021 Jan;42(1):44-8. [CrossRef] [PubMed] [PMC free article]
- Lee EY, Lee YH, Jin SM, Yang HK, Jung CH, Park CY, et al. Differential association of Body Mass Index on Glycemic Control in Type 1 Diabetes. Diabetes Metabolism Research and Reviews. 2017;33(1). doi: 10.1002/dmrr.2815. [CrossRef] [PubMed]
- Nansel TR, Lipsky LM, Iannotti RJ. Cross-sectional and Longitudinal Relationships of Body Mass Index with Glycemic Control in Children and Adolescents with Type 1 Diabetes Mellitus. Diabetes Research and Clinical Practice. 2013;100(1):126-32. [CrossRef] [PubMed] [PMC free article]
- Verma A, Rajput R, Verma S, Balania VKB, Jangra B. Impact of Lockdown in COVID-19 on Glycemic Control in Patients with Type 1 Diabetes Mellitus. Diabetes and Metabolic Syndrome.2020;14:1213-16. [CrossRef] [PubMed] [PMC free article]
- Shah N, Karguppikar M, Bhor S, Ladkat D, Khadilkar V, Khadilkar A. Impact of Lockdown for COVID-19 Pandemic in Indian Children and Youth with Type 1 Diabetes from Different Socio-economic Classes. Journal of Pediatric Endocrinology and Metabolism. 2020;34(2):217-23. [CrossRef] [PubMed]
- Predieri B, Leo F, Candia F, et al. Glycemic Control Improvement in Italian Children and Adolescents with Type 1 Diabetes Followed Through Telemedicine During Lockdown Due to the COVID-19 Pandemic. Front Endocrinology. 2020;11:595735. doi:10.3389/fendo.2020.59573. [CrossRef] [PubMed] [PMC free article]
- Barret CE, Koyama AK, Alvarez P, Chow W, Lundeen EA, Perrine CG, et al. Risk for Newly Diagnosed Diabetes > 30 Days After SARS-CoV-2 Infection Among Persons Aged < 18 Years-United States. Morbidity and Mortality Weekly Report.2022;71(2):59-65. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2024.32
|
| Cite this article as: | | Novina N, Moelyo A G, Nuraeni E, Mihardja M L, Ariefudin Y, Faisal F, Pulungan A B. The Impact of COVID-19 Pandemic on Glycemic Control’s Children with Type 1 Diabetes Mellitus: A Multicenter Study in West and Central Java, Indonesia. Pediatr Oncall J. 2024;21: 103-109. doi: 10.7199/ped.oncall.2024.32 |
|