Sumitra Venkatesh, Shakuntala Prabhu.
Division of Pediatric Cardiology, Department of Pediatrics, B J Wadia Hospital for Children, Mumbai.
ADDRESS FOR CORRESPONDENCE
Shakuntala Prabhu, Div. of Pediatric Cardiology, Dept. of Pediatrics, B.J.Wadia Hospital for Children, Mumbai.
Email: ssprabhu1@hotmail.com | Electrocardiography records the electrical activity of the heart and is a useful, though under-utilized investigation in pediatric practice. It supplements the information obtained by clinical examination and chest radiography. ECG helps mostly in the assessment of chamber size, arrhythmias and ischemia. There are many nuances to the pediatric ECG that relate to age-specific changes. These findings relate directly to changes in the myocardium and circulatory system as the individual matures from infancy to adulthood. A recent review of pediatric emergency department use reveals that the most common reasons for obtaining ECGs in children are chest pain, suspected dysrhythmias, seizure, syncope, drug exposure, electrical burns, electrolyte abnormalities, and abnormal physical examination findings. Although a complete review of ECG interpretation is beyond the scope of this article, the authors suggest the use of a systematic approach to ECG interpretation.
The limitations of pediatric ECG are as follows:
- Age dependent changes noted-no single set of criteria can be used for all ages.
- Chamber enlargement rules are used from adult experience.
- Poor sensitivity; e.g. A large VSD may not have large LV forces.
- Absence of specific guidelines for chest lead placements.
- Interpretation requires practice as there are no validated normograms for age.
- Congenital heart diseases have very few lesion specific changes on ECG.
Basics of recording and interpretation :
- Usual 12 lead ECG is not enough in pediatrics, V4R or V3R is necessary in cases of congenital heart disease.
- The placement of leads must be more proximal in children to avoid limb-motion artifacts.
- Standard gains of 10mm/mV is used. If the QRS voltage is very large, then the gain may be halved. Each small block is 1mm high and each large block represents 5mm (vertical block).
- The horizontal axis represents the length of each electrical event in time. Each small block measures 0.04seconds and a large block (comprising of 5 small ones) correlates to 0.20 seconds.
- Intervals are better hand-measured as the computerized systems are often in-accurate. The intervals increase with increasing age and reach adult values by 7-8 years of age.
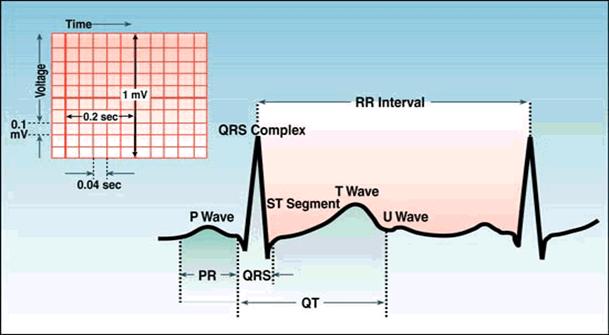
What does each wave represent ?
P wave represents atrial depolarization. This is the time taken by an electrical impulse to spread from the sino-atrial node through the atrial musculature. This wave precedes the QRS complex and is best measured in lead II.
The PR interval represents the time taken by an impulse to travel from the atria to the Purkinje fibres through the AV-node, bundle of His and the bundle branches. This is measured from the beginning of the P wave to the beginning of the QRS complex.
Q wave - Septal depolarization
RS wave - Ventricular depolarization
The QRS complex follows the PR interval and consists of 3 waves- the Q wave, R wave and S wave. The Q wave is always at the beginning of the QRS complex and may or may not be present. The R wave is the first positive deflection and is followed by the S wave which is a negative deflection.
The QT interval extends from the beginning of the QRS complex to the end of T wave and represents the time necessary for ventricular depolarization and repolarization. This interval is best measured in leads II, V5 and V6 and the longest interval is used.
The corrected QT interval or QTc is calculated by using Bazett's formula:
QTc = QT interval / Ö RR
The T wave represents ventricular repolarization and follows the S wave and S-T segment. At times, a U-wave follows the T wave and represents the repolarization of His and Purkinje fibres.
The electrocardiogram must be read systematically in the following order to extract the maximum information possible:
- Heart rate
- QRS axis
- Intervals-PR,QRS,QT/QTc
- P-wave amplitude and duration
- QRS and Q-wave amplitude ,R/S ratio
- S-T segment and T-wave
Rate calculation:
Heart rate = 1500 / Number of small squares in one R-R interval
Count the number of big boxes between the 2 R waves, if: 1= 300 bpm, 2 = 150 bpm, 3 = 100 bpm, 4 = 70 bpm and 5 = 60 bpm (bpm = beats per minute)
In children, cardiac output is determined primarily by heart rate as opposed to stroke volume. With age, the heart rate decreases as the ventricles mature and stroke volume plays a larger role in cardiac output. Age and activity-appropriate heart rates thus must be recognized. Average resting heart rate varies with age; newborns can range from 90-160 beats per minute (bpm) and adolescents from 50-120 bpm. The average heart rate peaks about the second month of life and thereafter gradually decreases until adolescence. Heart rates grossly outside the normal range for age should be scrutinized closely for dysrhythmias
Axis detection:
Axis helps to interpret the major vector of depolarization. Determine if the net QRS voltage is positive or negative in lead I and lead aVF. For example, if the R wave height is 10 mm (above the isoelectric line) and S wave height is 4 mm (below the isoelectric line), then the net QRS voltage is positive (+6). If the R wave is short and S wave is longer, the net QRS voltage would be negative.
The QRS axis can be located using the following simple rule: Lead I | Lead aVF | Interpretation | Comment | Positive | Positive | Normal axis | Abnormal in neonates and early infancy | Negative | Positive | Right axis deviation | Normal in neonates and in early infancy | Positive | Negative | Left axis deviation | Abnormal at any age | Negative | Negative | North-west axis | Abnormal at any age |
The Wave configuration:
Evaluate P wave in lead II and V1, if P wave is >2.5 boxes wide or tall, it is suggestive of left or right atrial enlargement respectively. LAE is denoted by 'wide and notched' P-waves and RAE is denoted by 'tall and peaked' P-waves. (Table 1)
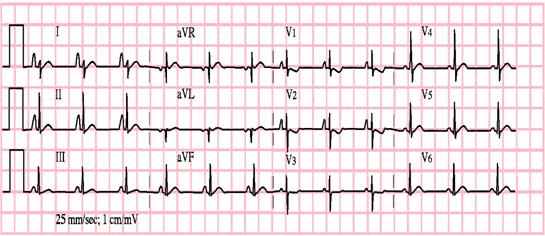
The RV hypertrophy or LV hypertrophy determination depends on the R-wave and S-wave voltages and their ratio (R/S). Tall R in V1 (R/S >1) with deep S in V6 and upright T waves in right precordial leads suggests RVH. Tall R in V5 and V6 with deep S in V1 and T wave abnormalities in V5 and V6 suggests LVH (Table 1).
Table 1. ECG criteria for ventricular and atrial hypertrophy:
Right ventricular hypertrophy | R wave greater than the 98 th percentile in lead V1 | S wave greater than the 98 th percentile in lead I or V6 | RSR' pattern in lead V1, with the R' height being greater than 15 mm in infants younger than 1 year of age or greater than 10 mm in children older than 1 year of age | Q wave in lead V1 | Left ventricular hypertrophy ( Fig 1) | R-wave amplitude greater than 98 th percentile in lead V5 or V6 | R wave less than 5 th percentile in lead V1 or V2 | S-wave amplitude greater than 98 th percentile in lead V1 | Q wave greater than 4 mm in lead V5 or V6 | Inverted T wave in lead V6 | | Right atrial enlargement ( Fig 2) | | Peaked P wave in leads II and V1 that is higher than 3 mm in infants younger than 6 months of age and greater than 2.5 mm in infants older than 6 months of age | | Left atrial enlargement | | P-wave duration greater than 0.08 seconds in a child younger than 12 months of age or greater than 10 ms in children 1 year and older | | P wave minimal or plateau contour | | Terminal or deeply inverted P wave in lead V1 or V3R | | The presence of any of these is suspicious for hypertrophy. It is not necessary for all of the criteria to be met. |
Figure 1. ECG tracing showing Left Ventricular Hypertrophy (LVH) with S in V1 deeper than 95% of normal and R in V6 taller than 95% of normal:
Figure 2. ECG tracing showing tall P waves suggestive of Right atrial enlargement:
S-T and T wave changes suggest ischemia or repolarization abnormalities. The elevation of ST-segment up to 1-4mm with the concavity facing upwards is normal. Any variation in the above depicts early repolarization, pericarditis, hyperkalemia, pneumothorax or pneumopericardium. ST depression is suggestive of pressure overload/strain.
In pediatric patients, T-wave changes on the ECG tend to be non-specific and are often a source of controversy. What is agreed on is that flat or inverted T waves are normal in the newborn. In fact, the T waves in leads V1 through V3 usually are inverted after the first week of life through the age of 8 years as the so-called "juvenile" T-wave pattern. Persistence of which suggests RVHT wave inversion in leads I, V5 and V6 is seen in ischemic conditions like ALCAPA, Kawasaki Disease and pressure overload/strain. Tall T wave suggests hyperkalemia and absent T-wave with U-wave suggests hypokalemia.
Normal variations to be considered in children (Table 2):
- Normal heart rate in the neonates varies between 120-230/min and gradually decreases over the first 6 months. Resting heart rate is about 120 beats/min at 1 year, 100 at 5 years and reaches adult values by 15 years.
- Appearance of secondary 'r' waves (r' or R') in right chest leads is normal in neonates.
- At birth, right axis deviation of the mean QRS vector is the rule. The axis becomes normal by 1 year of age. Hence, normal or leftward QRS axis is abnormal in the neonatal period and early infancy. Common conditions with leftward axis of QRS vector are tricuspid atresia and AV canal defects.
- The PR-interval varies with age. Neonates - 0.08-0.15, adolescents - 0.12-0.20 seconds. This normal variation must be kept in mind when considering diagnosis of conduction abnormalities or AV-blocks in children. Other pathological causes of short PR interval are Pompe's Disease, Fabry's disease, Mannosidosis, WPW syndrome, ectopic atrial pacemaker from lower right atrium.
- Dominant R in right precordial leads can persist up to 6 months to 8 years; in the majority, the R/S ratio in lead V1 becomes less than 1 by 4 years of age.
- Q waves are normally seen in leads II, III, aVF, V5 and V6 due to the clockwise loop of the QRS vector and are seen in majority of the congenital heart diseases. Q-waves in leads I and aVL suggest a counter-clockwise loop of the initial QRS vector and is seen in cases of Tricuspid atresia, Endocardial cushion defect and inlet VSD. Deep Q waves in lateral leads might point towards underlying anomalous origin of left coronary artery from pulmonary artery (ALCAPA).
- The QRS complex duration varies with age. In children, the QRS complex duration is shorter, possibly because of decreased muscle mass, and gradually increases with age. The QRS complex measures 0.03-0.08 seconds in neonates and 0.05-0.10 seconds in adolescents. As a result, slight prolongation of what may appear as a normal QRS complex can indicate a conduction abnormality or bundle branch block in children .
- QT interval is highly variable in the first 3 days of life and in early infancy may be as high as 0.49seconds. Corrected QT (calculated by Bazett's formula) of more than 0.44 seconds is abnormal thereafter. The common causes of prolonged QTc are hypokalemia, hypocalcemia, hypothermia and cerebral injury. Certain drugs also prolong the QT-interval, viz. cisapride, Macrolide antibiotics, etc.
- Preterms of < 28 weeks of gestation may not have right ventricular dominance. Chest leads may show LV dominance with normal or leftward QRS axis.
- Sinus pauses or junctional escapes (narrow QRS complex without preceding P waves) may occasionally occur during sleep, feeding and defecation.
Summary:
Interpreting pediatric ECG is easy if a systematic approach of heart rate, intervals, axis and waveform morphologies is applied. Knowing what is normal in pediatric age group helps to easily identify what is abnormal. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Sharieff GQ, Rao SO. The Pediatric ECG Emergency Medicine Clinics of North America. February 2006; 24(1):195-208. [CrossRef] [PubMed]
- H.D. H.P. E.B. Moss and Adams' heart disease in infants, children, and adolescents 6th edition. 2001Philadelphia: Lippincott, Williams and Wilkins.
- Park M.K., George R., Pediatric cardiology for practitioners. St. Louis: Mosby, 2002. p. 34-51.
- Savitsky E., Alejos J., Votey S., Emergency department presentations of pediatric congenital heart disease. J Emerg Med (2003) 24: 239-245. [CrossRef]
- Sharieff G., Wylie T., Pediatric cardiac disorders. J Emerg Med (2004) 26 : 65-79. [CrossRef] [PubMed]
- Schwartz PJ, Garson A, Paul T et al. Guidelines for the interpretation of the neonatal electrocardiogram. European Heart J 2002; 23:1329-44. [CrossRef]
- Horton L., Mosee S., Brenner J., Use of the electrocardiogram in a pediatric emergency department. Arch Pediatr Adolesc Med (1994) 148: 184-188. [CrossRef] [PubMed]
|
| Cite this article as: | | Venkatesh S, Prabhu S. Pediatric Electrocardiogram- The Basics. Pediatr Oncall J. 2007;4: 1-5. |
|