Moras KJ, Mundkur SC, George DM, Pereira RA.
Department of Paediatrics, Kasturba Medical College, Manipal Academy of Higher Education(MAHE), Manipal, Karnataka, India.
ADDRESS FOR CORRESPONDENCE
Mundkur SC, Professor and Head of the Unit, Department of Paediatrics, Kasturba Medical College, Manipal Academy of Higher Education,(MAHE)Manipal, Karnataka, India-576104.
Email: suneel_cm@hotmail.com. | | Abstract | | An 11-year-old male child presented with progressive back pain for 2 months and compression fracture of D7 vertebra. On examination, the child had no pallor, lymphadenopathy or organomegaly. The child had lower lumbar tenderness. Peripheral smear showed no blasts. Further investigations showed osteoporosis with compression fracture D7 to D11 vertebrae. Bone marrow aspiration confirmed the diagnosis of pre-B cell Acute Lymphoblastic Leukemia. | | | | Keywords | | Osteoporosis, Compression fracture vertebra, Pre-B cell Acute Lymphoblastic Leukemia. | | | | Introduction | | Osteoporosis is a condition of compromised bone strength due to loss of bone mineral density. Osteoporosis is uncommon in pediatric age group and is usually, secondary to malabsorption, chemotherapy, malignancy, prolonged corticosteroid treatment, rheumatic diseases, osteogenesis imperfecta and certain endocrine disorders. | | | | Case Report | An eleven-year-old boy presented with complaints of progressive lower back pain for two months which was limiting daily activities and causing difficulty in ambulation. The back pain increased on bending, walking, squatting and decreased at rest. No history of contact with tuberculosis. No other joint pain, swelling or morning stiffness. No history of pins and needles sensation. There was no history of fall. His bowel and bladder functions were normal. No recent history of weight loss, anorexia. fever, night sweats. He was on calcium and vitamin D supplements with no relief despite adequate milk intake. MRI spine done outside showed compression fracture of D7 vertebrae.
On examination, his vitals were HR-90/min, RR-15/min, BP-100/70mmHg, was afebrile; weight was 35 kg, height was 150 cms, BMI-15.5 kg/m2, SMR stage 1 no signs of pallor, petechiae, ecchymosis, lymphadenopathy or hepato-splenomegaly were found. Examination of the musculoskeletal system revealed tenderness over the lumbosacral region and restriction of movements of the lower spine. No swelling, gibbus or deformities of the spine noted. The power and reflexes of both lower limbs were normal. There was no bowel or bladder dysfunction. Other systemic examination was within normal limits.
Table 1. Laboratory investigations.
| ESR |
27 mm/hr |
(0-20 mm/hr) |
| CRP |
3 mg/L |
0-5 mg/L |
| Haemoglobin |
12.2 g/dl |
13-17 g/dl |
| Total WBC |
16.2 X 10³/µl |
4-10 X 10³/µl |
| Platelet Count |
287.0 x 10³/µL |
150-400 X 10³/µl |
| RBC Count |
4.57 x 10^6/µL |
4.5-7 x 10^6/µL |
| Peripheral smear |
Normocytic normochromic, no blasts |
|
| Total bilirubin |
0.9 mg/dL |
0.3-1.2 mg/dL |
| Direct bilirubin |
0.4 mg/dL |
0.0-0.4 mg/dL |
| AST |
46 IU/L |
15-40 IU/L |
| ALT |
44 IU/L |
17-63 IU/L |
| Albumin |
3.7 g/dL |
3.5-5 g/dL |
| Urea |
22 mg/dL; |
10-40 mg/dL |
| Creatinine |
0.56 mg/dL |
0.6-1.4 mg/dL |
| Sodium |
138 meq/L |
136-145 meq/L |
| Potassium |
4.3 meq/L |
3.5-5.1 meq/L |
| Calcium |
9.8 mg/dL |
8.2-10.2 mg/dL |
| Phosphorous |
6.8 mg/dL |
2.5-4.5 mg/dL |
| ALP |
242 IU/L |
40-130 IU/L |
| Uric acid |
3.8 mg/dl |
3.4-7 mg/dL |
| LDH |
252 U/L; |
200-450 U/L |
| Vitamin D(24,25-hydroxylase) |
30 ng/mL |
21-29 ng/mL |
| Parathyroid hormone |
9.5 pg/mL |
15-65 pg/mL |
| TSH |
3.3 µIU/mL; |
0.27-4.2 µIU/mL; |
| Prothrombin Time |
13.4 Sec |
11-13 s |
| INR |
1.20 |
0.9-1.1 |
| Tuberculin test |
negative |
|
The lateral spine radiograph showed osteopenia with multiple compression fractures of the thoracic vertebrae from D7 to D11. (Figure 1)
Figure 1. Compression fractures from D7 to D11vertebrae.
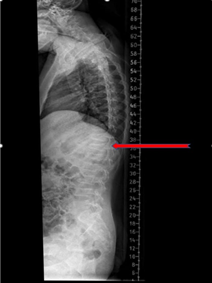
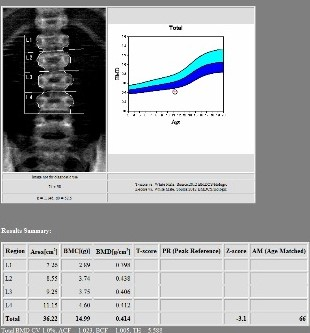
X-ray -Skull was showed no Wormian bones or punched-out lytic lesions. The pelvic radiograph showed generalized osteopenia. DEXA-scan did show a Z score of -3.1 in the lumbar vertebrae suggestive of osteoporosis. (Figure 2)
Figure 2. Lumbar vertebrae suggestive of osteoporosis.
USG abdomen done was unremarkable. Chest Xray showed no hilar lymphadenopathy and was not suggestive of pulmonary tuberculosis. Protein electrophoresis showed no evidence of M protein. A PET scan was done and showed no evidence of infection/neoplastic lesions.
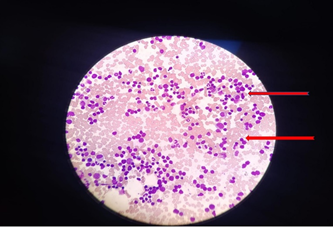
Bone marrow aspiration and biopsy were done which showed more than 50% blasts. (Figure 2) Flow cytometry was done on a bone marrow sample revealing pre-B-cell lymphoblastic leukemia. ( Figure 3) The child was treated in pediatric oncology for Leukemia.
Figure 3. Bone marrow aspiration showing lymphoblasts.
ACUTE LEUKEMIA PANEL
Clinical History: Compression fracture of vertebrae; ? malignancy; ? multiple myeloma
Specimen: Bone marrow aspirate
Blasts%: 56% (on morphology)
Flow cytometric immunophenotyping report
Descriptive Summary:
Immunophenotyping was done on bone marrow aspirate with low SSC and dim CD45+ events gated as blasts (89.7% of viable events)
Normal control population for gated events:
Negative: Normal lymphoid cells (low SSC, bright CD45+ events)
Blasts are positive for: CD34, CD19, CD20, CD10, CCD79a, HLADR
Blasts are negative for: CD3, cCD3, CD7, CD5, CD56, CCMPO, CD13, CD33, CD117, CD64, CD36, CD14, CD15, CD41
Flow cytometry was done on a bone marrow sample revealing pre-B-cell lymphoblastic leukemia. ( Figure 3)
| | | | Discussion | While primary causes of osteoporosis (osteogenesis imperfecta) are rare, the increase in the incidence of osteoporosis is due to acquired pathological causes (rheumatologic conditions). International Society for Clinical Densitometry (ISCD) Position Statement defined osteoporosis as “ A clinically significant fracture history (with one or more of the following): 1. a long bone fracture of the lower extremities 2. a vertebral compression fracture, 3. two or more long bone fracture of the upper extremities B. Low spinal or total body less head areal bone density or bone mineral content, defined as Z- score less than or equal to -2.0 adjusted for age, gender and body size, as appropriate.”1
Incidence of vertebral fracture is estimated to be 1-5% of all fractures occurring in children.2 Osteoporotic vertebral fracture are seen in osteogenesis imperfecta,3 inflammatory bowel disease, glucocorticoid use, acute lymphoblastic leukemia,4,5
Osteoporosis is a known complication of Paediatric Leukemia and can occur from the time of diagnosis to after remission. In a study done by Meera Rayar et al found that 11% of children with acute leukaemia had osteoporosis at time of diagnosis.6 Osteoporotic vertebral fracture in children with acute lymphoblastic leukaemia, typically reported after treatment with chemotherapy/glucocorticoids. Another study reported cumulative incidence of 32.5% of vertebral fracture over 6 years from diagnosis in a prospective Canadian cohort.5
However very few cases have been reported with acute onset osteoporosis and vertebral fracture resulting in diffuse back pain as the only presenting complain of acute lymphoblastic leukemia as seen in our case.
There are case reports of vertebral fracture, presenting as Leukemia.7,8 However, in these case reports, the peripheral smear, showed pancytopenia7 and neutropenia8, making bone marrow study the next step for arriving at diagnosis. In our patient, complete hemogram, ESR and peripheral smear were normal. Child was worked up for other causes of osteoporosis, like Langerhans Cell Histiocytosis, Osteogenesis imperfecta, Tuberculosis, Multiple myeloma which were negative. However, in view of high index of suspicion bone marrow studies were done which clinched diagnosis of Pre B Acute Lymphoblastic Leukemia.
| | | | Conclusion | | This case presents importance of detailed evaluation required in non co-morbid children presenting with acute onset osteoporosis. The correlation between osteoporosis and ALL needs to be studied. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Rauch F, Plotkin H, DiMeglio L. et al. Fracture prediction and the definition of osteoporosis in children and adolescents: the ISCD 2007 Pediatric Official Positions. J Clin Densitom. 2008;11:22-8. [CrossRef] [PubMed]
- Carreon LY, Glassman SD, Campbell MJ. Pediatric spine fractures: a review of 137 hospital admissions. J Spinal Disord Tech. 2004 Dec;17(6):477-82. doi: 10.1097/01.bsd.0000132290.50455.99. PMID: 15570118. [CrossRef] [PubMed]
- BishopN(2010)Characterising and treating Osteogenesis Imperfecta.EarlyHumDev86:743-74602. [CrossRef] [PubMed]
- MäkitieO(2013)Causes,Mechanisms and Management of Paediatric Osteoporosis.NatRevRheumatol9:465-475. [CrossRef] [PubMed]
- Ward LM, Ma J, Lang B, et.al; Steroid-Associated Osteoporosis in the Pediatric Population (STOPP) Consortium. Bone Morbidity and Recovery in Children With Acute Lymphoblastic Leukemia: Results of a Six-Year Prospective Cohort Study. J Bone Miner Res. 2018 Aug;33(8):1435-1443. doi: 10.1002/jbmr.3447. Epub 2018 May 22. PMID: 29786884. [CrossRef] [PubMed]
- Rayar MS1, Nayiager T, Webber CE, et al Predictors of Osteopenia/Osteoporosis in Children with Acute Lymphoblastic Leukemia. Pediatr Blood Cancer. 2012 Jul 15;59(1):77-82. doi: 10.1002/pbc.24040. [CrossRef] [PubMed]
- Salim H, Ariawati K, Suryawan WB, et.al.Osteoporosis resulting from acute lymphoblastic leukemia in a 7-year-old boy: a case report. J Med Case Rep. 2014 May 28;8:168. doi: 10.1186/1752-1947-8-168. PMID: 24885558; PMCID: PMC4077677. [CrossRef] [PubMed] [PMC free article]
- Vasikaran SM, Patel SM, Cambara A. Finding the "B" in Bone Loss: Osteoporosis as the Preceding Symptom of B Cell Acute Lymphoblastic Leukemia | Pediatrics | American Academy of Pediatrics [Internet]. American Academy of Pediatrics. 2022 [cited 2022 Oct 18].
DOI: https://doi.org/10.7199/ped.oncall.2025.45
|
| Cite this article as: | | Moras K J, Mundkur S C, George D M, Pereira R A. Osteoporosis in an 11 year old: a case report. Pediatr Oncall J. 2025;22. doi: 10.7199/ped.oncall.2025.45 |
|