Reena Jain, Parminder Kaur, Pankaj Kumar, Vishal Guglani, Shivani Randev.
Department of pediatrics, Government Medical College and Hospital, Chandigarh, India.
ADDRESS FOR CORRESPONDENCE
Dr. Shivani Randev, Department of Pediatrics, Government Medical College and Hospital Sec 32B, Chandigarh 160047.
Email: shivanirandev@hotmail.com. | | Abstract | Background: Acute febrile thrombocytopenia is a commonly encountered entity in hospitalized patients. The usual etiology in tropical countries is an infection, though the common etiological agents will vary depending upon the region and season. Accurate and early diagnosis, though challenging at times, is important as timely institution of appropriate treatment may be life-saving. This study was planned to evaluate the clinical and etiological profile of pediatric patients admitted with acute febrile thrombocytopenia and to assess their complications and outcome.
Patients and Methods: A retrospective study of hospital records of 118 patients with acute febrile thrombocytopenia was carried out. Their clinical findings, investigations and outcome were recorded and analyzed.
Observations: An etiological diagnosis could be made in 81% patients. The most common etiology was scrub typhus (44%) followed by dengue fever (11%). Lower platelet counts were associated with a higher risk of complications like shock, acute kidney injury, encephalopathy and bleeding manifestations. Of all enrolled patients, 108 recovered and were discharged while 7 patients died and 3 left against medical advice.
Conclusion: Infectious illnesses are commonest causes of acute febrile thrombocytopenia. Knowing the common etiological profile in a particular region and season will help in timely institution of appropriate empiric therapy to reduce morbidity and mortality from the condition. | | | | Keywords | | scrub typhus, dengue, malaria, sepsis, enteric fever. | | | | Introduction | Thrombocytopenia is defined as an abnormal decrease in platelet count below the lower limit of normal which is taken as 150,000 lac/microliter (mcL).1,2 Various infectious and non-infectious causes may act in more than one way resulting in a lower than normal platelet count. Infectious causes include tropical infections (malaria, dengue, rickettsial fever, Hanta virus, Lassa virus) and other infections like typhoid and sepsis. Non-infectious thrombocytopenia can occur due to increased destruction of platelets (Idiopathic thrombocytopenic purpura (ITP), Thrombotic thrombocytopenic Purpura (TTP), Hemolytic uremic syndrome (HUS), Paroxysmal nocturnal hemoglobinuria (PNH), Systemic lupus erythematosus), decreased production (vitamin B12, folate deficiency and leukemia) and drug induced (quinine, valproate, methotrexate, isotretinoin, heparin), (Table 1).1,2 It is important to determine the etiology for the condition, as timely institution of appropriate therapy may be lifesaving.
The symptomatology of thrombocytopenia may range from being asymptomatic and incidentally discovered to severe life threatening gastrointestinal or central nervous system bleed.3 The decrease in platelet count is directly related to the risk of severe bleeding and further complications. Hence, it is of utmost importance to serially monitor the platelet count and to determine the cause of febrile thrombocytopenia.
In tropical countries like India, infections are the leading cause of febrile thrombocytopenia, as the climate is favourable for various vectors. A systematic approach in diagnosing the cause of acute febrile thrombocytopenia helps in prompt treatment and lower morbidity and mortality. Many previous studies have been done to study the clinical and etiological profile of febrile thrombocytopenia in adult patients in various parts of the country. This study is intended to describe the clinical profile of children with acute febrile thrombocytopenia and to analyze the leading causes of infectious disease associated with acute febrile thrombocytopenia in children. Knowing the leading causes of acute febrile thrombocytopenia can help in administering the empirical therapy at the earliest and improving the outcome. It will also allow us to institute appropriate epidemiological measures at community level.
Table 1. Causes of decreased platelet count1,2
| Decreased production |
Vitamin B12 and folate deficiency,
Leukaemia |
Sepsis
Hereditary disease |
| Increased destruction |
Idiopathic thrombocytopenic purpura (ITP),
Thrombotic thrombocytopenic Purpura (TTP),
Hemolytic uremic syndrome (HUS),
Disseminated intravascular coagulation (DIC) |
Paroxysmal nocturnal hemoglobinuria (PNH),
Systemic lupus erythematosus(SLE), antiphospholipid syndrome, post-transfusion purpura and hypersplenism |
| Drugs |
Quinine,
Valproic acid,
Methotrexate,
Carboplatin |
Interferon,
Isotretinoin and
Heparin |
| Infections |
Malaria,
Leptospirosis,
Rickettsial infections,
Septicemia,
Typhoid,
Borreliosis |
Arbovirus diseases such as dengue or yellow fever, rodent-borne viruses (Hanta and Lassa fever),
Visceral leishmaniasis |
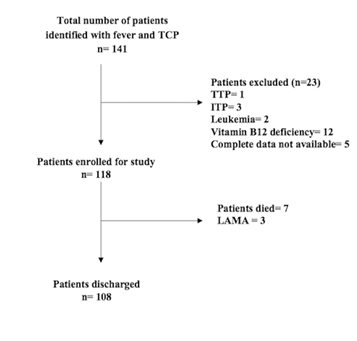
| | | | Methodology | We conducted a retrospective observational study in the Department of Paediatrics, at tertiary care hospital in Chandigarh after from the institutional ethics committee. All children, 1 month to 14 years of age who were admitted to paediatric emergency between April 2019 to April 2020 with a history of fever (skin temperature >37.2 degree Celcius) of less than 2 weeks duration and thrombocytopenia (platelet count less than 150,000/mcL) were considered for enrolment. Febrile children who were known cases of TTP (Thrombotic Thrombocytopenic Purpura), ITP (Immune Thrombocytopenic Purpura), malignancies on chemotherapy or those in whom thrombocytopenia was attributed to vitamin B12 or folate deficiency were excluded from the study (Figure 1). For all eligible children (118 cases), clinical data was retrieved from the medical records and noted on a pre-designed proforma which included information on their clinical profile, laboratory parameters, etiological profile, complications and outcomes. The final diagnosis was based on the clinical and laboratory parameters. Investigations like complete blood count, liver and kidney function tests and fever work up including scrub typhus serology, dengue antigen test and serology, peripheral blood film, rapid malarial antigen test, widal test and blood culture were recorded for all patients.
Statistical analysis: Continuous variables are expressed as mean and standard deviation/median. Categorical variables are reported as numbers and proportions.
Figure 1. Flow chart of patient enrolment.
 | | | | Results | A total of 118 patients with febrile thrombocytopenia were enrolled over a period of one year. The patients’ ages ranged from 9 months to 14 years, out of which 56% patients were in the age group of (6-10 years) followed by 19% in the age group (11-14 years). Out of 118 patients 67 (56.7%) were males and 51 (43.3%) were females (Table 2). Most patients of febrile thrombocytopenia were admitted between July to September (43.2%) followed by October to December months (27.9%), which corresponds with monsoon and post monsoon season. The commonest symptom after fever was gastric upset (pain abdomen/vomiting) in 46 patients (39%), followed by respiratory distress (9.3%), seizures and altered sensorium (8.5%), oedema (4.2%) and headache (2.5%).
Thrombocytopenia of platelet count less than 20,000/mcL was found in 9 patients (7.6%), out of which 5 patients had gastrointestinal bleeding. Platelet count in the range of 20,000-50,000/mcL was seen in 33 patients (28%), out of which 9 patients had either mucosal bleed or petechial rash. Platelet count in the range of 50,000-100,000/mcL was present in 44 (37.3%) and between 100,000-150,000/mcL in 32 patients (27.1%), without any bleeding manifestations. Hepatitis with raised transaminases and Acute Kidney Injury (AKI) were reported in 72 (61%) and 16 (13.5%) patients respectively. Other complications observed were shock (25.4%), encephalopathy (7.6%), meningitis (2.5%) and Acute Respiratory Distress Syndrome (ARDS) in 6% of patients.
As shown in Table 3, the commonest cause of febrile thrombocytopenia was found to be Scrub Typhus (44%) in our study, followed by Dengue (11.8%), Malaria (9.3%), Sepsis (9.3%) and Enteric Fever (5%). Out of 118 patients the exact cause could not be identified in 23 patients (19.5%), these patients had mild symptomatology and all of them improved. Three patients had mixed infections, dengue with scrub typhus in 2 patients and enteric fever with scrub typhus in one. Severe thrombocytopenia (Platelet count <50,000/mcL) was seen most commonly in scrub typhus and dengue. The rate of all complications like shock, AKI, encephalopathy, ARDS and bleeding was higher amongst patients with severe thrombocytopenia, however, no such co relation was seen with complications like hepatitis and meningitis (Table 3).
Out of 118 patients, 108 patients improved and were discharged, while 7 patients died and 3 patients left against medical advice. Among 7 patients who died, 4 were diagnosed with scrub typhus, one with dengue, one with malaria and one had sepsis with multiorgan dysfunction and Disseminated Intravacular Coagulation (DIC). Shock was seen in 5 patients, hepatitis and AKI in 5 and 3 patients, respectively. One patient had scrub typhus with encephalitis and one patient had ARDS. Two patients had platelet count <20,000/mcL, three patients had platelet count in between 20,000-50,000/mcL and two patients in the range of 50,000-100,000/mcL (Table 3).
Out of 52 scrub typhus patients 25 were males and 27 were females, ages ranging from 1-14 years. Platelet count of less than 20,000/mcL was observed in 4 patients, 3 of whom had gastrointestinal bleeding. Platelet count was in the range of 20,000-50,000/mcL in 16 patients, 6 of whom had petechial or mucosal bleed. Complications observed among scrub typhus patients were hepatitis (42, 80.77%), shock (14, 26.92%), encephalopathy/meningitis (11, 21.15%), AKI (7, 13.46%) and ARDS (3, 5.77%).
Table 2. Preliminary data of study patients.
| Total number of patients |
N=118 |
Percentage |
| Male |
67 |
56.7% |
| Female |
51 |
43.3% |
| Age distribution |
|
|
| 1 month to 5 years |
29 |
24.5% |
| 6-10 years |
66 |
56% |
| 11-14 years |
23 |
19.5% |
| Month wise distribution |
|
|
| April to June |
21 |
17.8% |
| July to September |
51 |
43.2% |
| October to December |
33 |
27.9% |
| January to march |
13 |
11.1% |
| Clinical signs and symptoms |
|
|
| Fever |
118 |
100% |
| Pain abdomen |
28 |
24% |
| Vomiting |
18 |
15.2% |
| Respiratory distress |
11 |
9.3% |
| Edema and anasarca |
5 |
4.2% |
| Seizures |
6 |
5.0% |
| Altered sensorium |
4 |
3.4% |
| Headache |
3 |
2.5% |
| Hepatospleenomegaly |
20 |
17% |
| Hepatomegaly |
15 |
12.7% |
| Splenomegaly |
4 |
3.4% |
| Jaundice |
4 |
3.4% |
| Platelet count distribution |
|
|
| 100,000-150,000/mcL |
32 |
27.1% |
| 50,000-100,000/mcL |
44 |
37.3% |
| 20,000-50000/mcL |
33 |
28.0% |
| <20,000/mcL |
9 |
7.6% |
| Bleeding manifestations |
|
|
| Petechiae |
4 |
3.4% |
| Mucosal bleed (nose or mouth) |
5 |
4.2% |
| Gastrointestinal bleed |
5 |
4.2% |
| Complications |
|
|
| Hepatitis |
72 |
61.0% |
| Shock |
30 |
25.4% |
| AKI |
16 |
13.5% |
| Encephalopathy |
9 |
7.6% |
| Meningitis |
3 |
2.5% |
| ARDS |
7 |
6.0% |
| Outcomes |
|
|
| Improved and discharged |
108 |
91.5% |
| Died |
7 |
6.0% |
| LAMA |
3 |
2.5% |
Table 3. Etiological distribution, complications and outcomes association with degree of thrombocytopenia.
| Etiology |
Proportion of total cases
N=118 |
Platelet count
100,000-150,000/mcL
n=32 |
Platelet count
50,000-100,000/mcL
n=44 |
Platelet count
20,000-50000/mcL
n=33 |
Platelet count
<20,000/mcL
n=9 |
| Scrub typhus |
52 (44%) |
11 |
21 |
16 |
4 |
| Dengue |
14 (11.8%) |
3 |
3 |
5 |
3 |
| Malaria |
11 (9.3%) |
2 |
5 |
3 |
1 |
| Sepsis |
11 (9.3%) |
1 |
5 |
4 |
1 |
| Enteric |
4 (3.3%) |
2 |
1 |
1 |
0 |
| Mixed |
3 (2.5%) |
0 |
0 |
3 |
0 |
| Unidentified |
23 (19.5%) |
13 |
9 |
1 |
0 |
| Complications |
| Hepatitis |
72 (61.0%) |
18 (56%) |
25 (56%) |
24 (72%) |
5 (55%) |
| Shock |
30 (25.4%) |
7 (21.8%) |
11 (25%) |
9 (27%) |
3 (33.3%) |
| AKI |
16 (13.5%) |
1 (3.1%) |
8 (18.1%) |
5 (15%) |
2 (22.25%) |
| Encephalopathy |
9 (7.6%) |
3 (9.3%) |
2 (4.5%) |
3 (9%) |
1 (11.1%) |
| Meningitis |
3 (2.5%) |
1 (3.1%) |
1 (2.2%) |
1 (3%) |
0 |
| ARDS |
7 (6.0%) |
0 |
4 (9%) |
1 (3%) |
2 (22.2%) |
| Bleeding manifestations |
14 (11.8%)) |
0 |
0 |
9 (27%) |
5 (55%) |
| Outcomes |
| Discharged |
108 (91.5%) |
31 (96%) |
43 (98%) |
31 (94%) |
3 (33%) |
| Died |
7 (6.0%) |
0 |
2 (4.5%) |
3 (9%) |
2 (22%) |
| LAMA |
3 (2.5%) |
1 |
1 |
0 |
1 |
| | | | Discussion | Acute febrile thrombocytopenia is a commonly encountered problem in tropical countries, mostly during monsoon season. Most commonly, infections (viruses, bacteria, rickettsia and protozoa) have been implicated as causative agents, because non-infectious causes of thrombocytopenia does not necessarily present with fever. Few cases of megaloblastic anaemia due to vitamin B12 or folate deficiency and leukemia may present with fever and thrombocytopenia. In such cases complete blood count and peripheral smear showing anaemia and low blood counts can help in making the primary diagnosis. Patients with ITP and TTP usually presents with increased bleeding tendencies without any fever. Also, patients receiving any drugs leading to thrombocytopenia can be elicited in history itself. Hence, in studies including febrile thrombocytopenia non-infectious causes of thrombocytopenia are rarely encountered. In a prospective cross sectional study out of 393 patients with febrile thrombocytopenia only 22 patients (5%) were diagnosed to have non-infectious causes including leukemia and vitamin B12 deficiency, while rest 95% patients had infectious thrombocytopenia.4 In this study already diagnosed cases of platelet dysfunction, leukemia and patients taking immunosuppressive drugs were excluded on the basis of history. Similarly such cases were excluded in the present study on the basis of history and preliminary investigations.
In the present study, the most common infective cause of acute febrile thrombocytopenia was scrub typhus (44%), accounting for almost half of the cases. Scrub typhus is a zoonotic disease caused by Orientia tsusugamushi and is frequently associated with thrombocytopenia. In a previous study from Chandigarh, thrombocytopenia was found in 90% of children with scrub typhus, while in in another study from Uttrakhand, it was seen in 80% cases.5,6 Various factors which have been implicated in causing thrombocytopenia in scrub typhus are dic, endothelial dysfunction with vasculitis and thrombus formation and immune mediated destruction.7
Dengue fever was the second most common (11.8%) cause of acute febrile thrombocytopenia in our patients. Thrombocytopenia in viral infections may occur due to invasion by the virus or toxic effects of viral proteins leading to decreased platelet production. There can also be increased peripheral platelet destruction via virus induced antibodies or antigen antibody complexes.8,9,10 In our study, malaria was found in 9.3% of patients (all were Plasmodium vivax). Immune mediated destruction with splenic sequestration and platelet consumption by dic are the mechanisms causing thrombocytopenia in malaria.11 In malaria, mild to moderate thrombocytopenia is more commonly documented than severe thrombocytopenia12, as seen in our study also. Several other studies (in paediatric as well as adult patients) have shown either malaria12,13,14 or dengue15,16,17,18 as the commonest aetiology leading to febrile thrombocytopenia with majority cases in monsoon and early winter season.
Sepsis was the diagnosis in 11 (9.3%) patients in the present study, out of which 2 were blood culture positive, while the rest were diagnosed on clinical grounds. In sepsis, thrombocytopenia is mainly attributed to dic, while other mechanisms like hemophagocytosis of megakaryocytes in bone marrow and direct platelet toxicity by microorganisms also play a role.19 A previous study in adult population by Nair et al have shown sepsis as the commonest cause of febrile thrombocytopenia.20
Enteric fever has been reported as one of the causes of febrile thrombocytopenia, the percentage ranged from 7% to 26% of total febrile thrombocytopenia cases in different studies.21,22,23,24 Also, decreased platelet count in enteric fever is considered as a marker of severe disease with complications.21 In our study, only 4.2% of patients had typhoid and majority of them had mild to moderate thrombocytopenia, similar to that reported in other studies.
Bleeding manifestations were seen in 11.8% of the patients, similar to that reported by Kumar P et al14, while Nair et al20 and Ramabhatta et al15 observed bleeding in 40% and 28.4% of thrombocytopenic patients, respectively. Severe thrombocytopenia (<20,000/mcL) was seen in 5% patients in our study similar to the study by Ramabhatta et al15 (8%). The rate of complications increased with severity of thrombocytopenia.
| | | | Conclusion | | Febrile thrombocytopenia is a common entity with a varied etiological profile. A systematic approach of investigations can help in making an early diagnosis and timely institution of appropriate treatment. In our study, scrub typhus was the commonest cause of infections associated with acute febrile thrombocytopenia, which can be due to nearby hilly areas and high incidence of scrub typhus in rainy seasons in this region. However, the commonest cause can vary from place to place and is related to endemicity of the disease. The limitation of our study is that it is a single center hospital based observational study which represents only the north Indian region. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Bichile SK. Platelet disorder. API Textbook of Medicine. Vol. 1, 9th edition, Munjal YP (Ed.), Jaypee Brothers: New Delhi 2012; 987-988.
- Lee GR, Foerster J, Lukens J, Paraskevas F, Greer JP, Rodgers GM. Shirley Parker Levine-Miscellaneous causes of thrombocytopenia. Wintrobe's Clinical Haematology. Lipincott Williams: Philadelphia 1999:10(2); 1623-1629.
- Konkle BA. Disorders of platelets and vessel wall. Harrison's Principles of Internal Medicine. Fauci AS, Braunwald E, Kasper DL, et al. (Eds.), McGraw-Hill: New York, 2008:17(1);718-23.
- Modi TN, Mehta AD, Sriram AS. Clinical profile of febrile thrombocytopenia: a hospital-based cross-sectional study. J Res Med Den Sci 2016;4(2):115-120. [CrossRef]
- Sharma N, Biswal M, Kumar A, Zaman K, Jain S, Bhalla A. Scrub Typhus in a Tertiary Care Hospital in North India. Am J Trop Med Hyg. 2016;95(2):447-51. [CrossRef] [PubMed] [PMC free article]
- Bhargava A, Kaushik R, Kaushik RM, et al. Scrub typhus in Uttarakhand & adjoining Uttar Pradesh: Seasonality, clinical presentations & predictors of mortality. Indian J Med Res. 2016;144(6):901-909. [CrossRef] [PubMed] [PMC free article]
- Lee HJ, Park CY, Park SG, Yoon NR, Kim DM, Chung CH. Activation of the coagulation cascade in patients with scrub typhus. Diagn Microbiol Infect Dis. 2017;89(1):1-6. [CrossRef] [PubMed]
- Assinger A. Platelets and infection - an emerging role of platelets in viral infection. Front Immunol. 2014;18;5:649. [CrossRef] [PubMed] [PMC free article]
- Ganesan N, Gunasekharan I and Padhi S. Platelet phagocytosis in peripheral blood during acute phase of dengue virus infection. J Curr Res Sci Med 2015; 1:51-53.
- Jayashree K, Manasa GC, Pallavi P, Manjunath GV. Evaluation of platelets as predictive parameters in Dengue fever. Indian Journal Hematol Blood Transfusion; 2011;27(3):127-30. [CrossRef] [PubMed] [PMC free article]
- Patel U, Gandhi G, Freidman S, Niranjan S. Thrombocytopenia in Malaria. J Natl Med Assoc 2004; 96(9):1212-4.
- Shetty G, Avabratha KS, Gonsalves S, Dany A, Rai BS. Thrombocytopenia in children with malaria-A study from coastal Karnataka, India. Asian Pacific Journal of Tropical Disease. 2012;2(2):107- 109. [CrossRef]
- Morales AJR, Sanchez E, Vargas M, Piccolo C, Colina R, Marria- Anemia and thrombocytopenia in children with Plasmodium Vivax malaria, Journal of Tropical Paediatrics 2006;52(1):49-51. [CrossRef] [PubMed]
- Kumar P, Chandra K. A clinical study of febrile thrombocytopenia- A hospital based retrospective study, Indian Journal of Clinical Practice. 2014; 24(10):952-957.
- Ramabhatta S, Kariyappa P, Kondappa B, Rao U.K, SanikamH. An aetiological profile of febrile thrombocytopenia in children. Sri Lanka Journal of Child Health, 2018; 47(2): 146-148. [CrossRef]
- Shankar RR, Kambdar PK, Dabhi AS. Clinical and laboratory evaluation of patients with fever with thrombocytopenia. Indian Journal of Clinical Practice. 2013;24:360-3.
- Masamatti SS, Vijaya C, Bhat A. Laboratory and etiological profile of febrile thrombocytopenia cases A cross sectional study. National Journal of Laboratory Medicine. 2016; 5 (3):44-8.
- Bhatnagar MK, Yadav SK, Jagdish RK. Clinical, haematological and biochemical profile in acute febrile illnesses with thrombocytopenia. International Journal of Medical Science and Clinical Invention. 2016; 3(10):2207-2213. [CrossRef]
- Lee GR, Foerster J, Lukens J, Paraskevas F, Greer JP, and Rodgers GM. Miscellaneous causes of Thrombocytopenia. Wintrobe's clinical hematology. 10th edition:1623-29.
- Nair PS, Jain A, Khanduri U and Kumar V. A Study of fever associated with thrombocytopenia. JAPI 2003; 51:1173.
- Herbinger KH, Schunk M, Nothdruft HD, Von Sonnenburg F, Loscher T, Bretzel G. A comparative study on infection induced thrombocytopenia among returned travellers. Infection. 2012;40(4):373-9. [CrossRef] [PubMed]
- Malik AS. Complications of bacteriologically confirmed typhoid fever in children, Journal of Tropical Paediatrics. 2002; 48 :102-8. [CrossRef] [PubMed]
- Chandrashekar, Anilkumar YC, Kirandeep S, Dalal SS. A study of clinical and laboratory profile of enteric fever in paediatric age group. Int J of Basic and Applied Med Sciences. 2013:3(3):16-23.
- Ahmed Y, Idris Y, Sehahatti K. Clinical and laboratory presentation of typhoid fever. International Pediatrics. 2001;16(4):227-31.
DOI: https://doi.org/10.7199/ped.oncall.2024.21
|
| Cite this article as: | | Jain R, Kaur P, Kumar P, Guglani V, Randev S. Clinico-etiological profile and outcome of children with acute febrile thrombocytopenia caused by various infections. Pediatr Oncall J. 2024;21: 7-12. doi: 10.7199/ped.oncall.2024.21 |
|