Joana Filipe Ribeiro1, João Virtuoso1, Ana Pinto2, Rita S. Oliveira1, Joana Ferreira2, Manuel Salgado3.
1Serviço de Pediatria, Hospital Sousa Martins, ULS Guarda, Guarda, Portugal,
2Serviço de Reumatologia, Hospital Sousa Martins, ULS Guarda, Guarda, Portugal,
3Unidade de Reumatologia Pediátrica, Hospital Pediátrico de Coimbra, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal.
ADDRESS FOR CORRESPONDENCE
Joana Filipe Ribeiro, Department of Pediatrics, Hospital Sousa Martins, Unidade Local de Saúde da Guarda Av. Rainha Dona Amélia 19, 6300-749 Guarda, Portugal.
Email: joanafiliperibeiro@gmail.com. | | Abstract | | Henoch-Schönlein Purpura (HSP) is an acute, systemic, immune complex-mediated leukocytoclastic vasculitis and the most common vasculitis of childhood. HSP is typically self-limited, although some patients experience one or more recurrences. We presented a 16-year-old male, with palpable purpura, abdominal pain and arthralgia, who was diagnosed with HSP. Due to intense and persisting abdominal pain, a high-dose oral prednisolone was initiated, resulting in clinical improvement. However, every attempt at weans off of prednisolone resulted in disease relapse. Combination therapy with colchicine allowed the discontinuation of corticosteroid therapy and no relapses of the disease was observed. The management of HSP cases with an unusual and complicated presentation remains controversial. However, several cases of successful treatment using immunomodulatory therapy have been reported. The use of colchicine has enabled the successful tapering off prednisolone, reduced its side effects and prevented further recurrences. | | | | Keywords | | Vasculitis, Henoch-Schönlein Purpura, Relapse, colchicine. | | | | Case Report | A 16-year-old male patient presented to the pediatric emergency department with a 48-hour history of severe abdominal pain, rash and arthralgia in his lower limbs, along with fresh blood in his stools. He had no relevant past medical history as well as no family history of autoimmune diseases. Physical examination revealed several, symmetrical, non-painful, palpable purpuric lesions on abdomen and both anterior and posterior sides of his legs (Figure 1), but was otherwise unremarkable. Initial blood workup showed normal complete blood count and inflammatory markers, but a positive IgM serology for Mycoplasma Pneumoniae (MP) and negative IgG. Autoimmune screening and remaining serologies were unremarkable (Table 1). The urine analysis revealed leukocyturia (leukocytes >20 cells/ field) and hematuria (erythrocytes 70 /uL) and abdominal ultrasound was normal.
Henoch-Schönlein Purpura (HSP) was diagnosed and due to intense abdominal pain, that persisted even after optimization of analgesics, the patient was hospitalized. He initiated on high-dose oral prednisolone (60 mg/day) and a 10-day course of clarithromycin, based on MP serology. Skin biopsy revealed a leukocytoclastic vasculitis. A good clinical outcome was achieved, with regression of purpuric lesions observed within a few days and the patient was discharged home on a prednisolone tapering regimen. Over the next five months, attempts to wean off prednisolone resulted in disease relapse, characterized by severe abdominal pain, arthralgia and widespread reappearance of the purpuric rash. Some episodes required hospitalization for pain management.
Following a comprehensive multidisciplinary team discussion, including Pediatric Rheumatologists, combination therapy with colchicine was initiated to achieve a gradual taper of steroids. Over a 12-month follow-up period, the patient showed favorable clinical evolution with no new recurrences episodes and it was possible to discontinue both corticosteroid therapy and colchicine. Notably, due to refractoriness to corticosteroid and the positive response to colchicine, the most frequent mutations in the MEFV gene were analyzed, but no pathogenic alterations were identified. Currently, the patient is already twenty years-old and no recurrences have been registered.
Figure 1. Palpable purpuric lesions on abdominal region and anterior aspects of both legs.
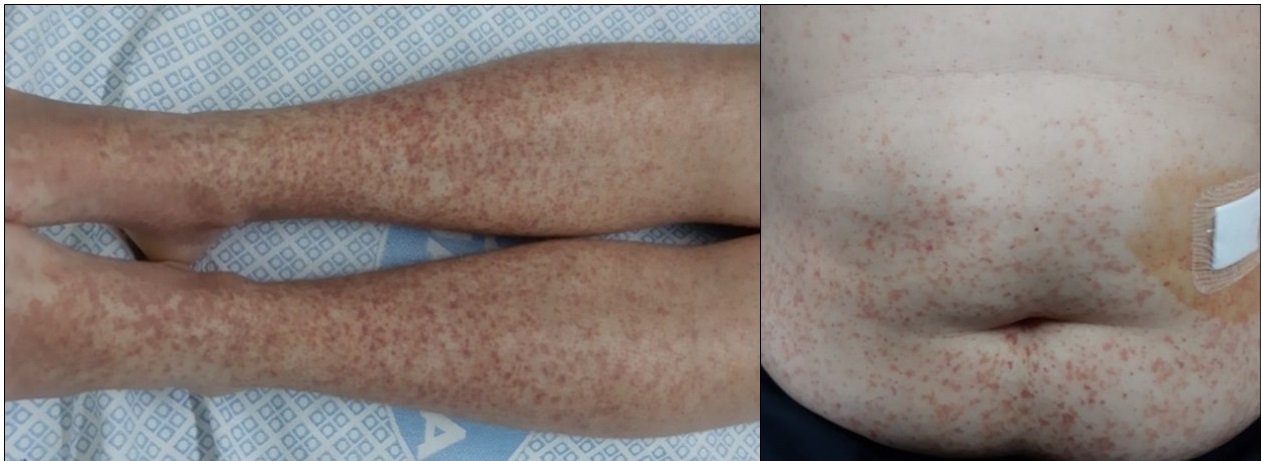
Table 1. Autoimmune screening and serology findings.
| Autoimmune Screening |
| ANA |
Negative |
| ANCA MPO |
Negative |
| ANCA PR3 |
Negative |
| Serologies |
| Cytomegalovirus |
IgG Positive/ IgM Negative |
| Epstein Barr Virus (IgM) |
IgM Negative |
| HIV I/II |
Negative |
| AgHbs |
Negative |
| AcHCV |
Negative |
| Ac. Anti HAV (IgM) |
IgM Negative |
| Ac. Anti-Mycoplasma Pneumoniae |
IgG Negative/ IgM Positive |
| Ac. Anti-Parvovirus |
IgG Negative/IgM Negative |
| | | | Discussion | HSP, also known as IgA Vasculitis, is a leukocytoclastic vasculitis characterized by the deposition of IgA complexes in the small vessels of the skin, joints, gastrointestinal tract and kidney. It is the most common vasculitis of childhood, usually presenting as a benign and self-limiting condition, with an incidence of 14-20/100,000 children, a slight male predominance and 90% of cases occurring between 3 and 10 years of age.1 Although less frequent in adults, complications in this age group tend to be more severe and chronic. The etiology remains unknown but several stimuli have been considered as possible triggers, like infections (Streptococcus ß- hemolytic, Adenovirus, Mycoplasma).1 Moreover, an increased risk of HSP has been described in familial Mediterranean fever, recurrent febrile syndromes and complement deficits.1
HSP diagnosis requires palpable purpura (without thrombocytopenia or coagulopathy) accompanied by at least one of the following: arthritis/arthralgia, diffuse abdominal pain, renal involvement or histopathological evidence of IgA deposits on skin/ kidney.2,3 Palpable purpura is typically symmetrical and mainly located on the back, gluteal region and lower limbs.2 Arthritis/arthralgias, the second most common manifestation (65% of cases), are transitory, migratory with oligoarticular involvement, mostly affecting the large lower limb joints.2 In half of the patients there is gastrointestinal involvement (GI), probably related to vasculitis, involving the splanchnic circulation (mesenteric vasculitis). As a result, patients main complaint is cramp-like abdominal pain and also nausea, vomiting, hematemesis, melena, hematochezia and, less frequently, invagination (ileo-ileal) and ischemic necrosis of the intestinal wall.2 In some patients, GI manifestation may precede the appearance of purpura. Renal involvement (20-54% of cases) is the most crucial prognostic factor and independently predicting morbidity and mortality. The clinical presentation can be heterogeneous, ranging from microscopic haematuria and proteinuria, to gross haematuria or even nephrotic syndrome. Purpura lasting more than 1 month or with recurrent episodes is more frequently associated with nephritis.2,4,5
Approximately 30% of patients with HSP experience relapses.2,3 Supportive care, including adequate hydration, rest and analgesia is the primary treatment approach. Non-steroidal anti-inflammatory drugs (NSAIDs) can be used for mild to moderate pain. However, in some individuals, especially those with recurrent episodes or complications, other interventions may be necessary. Systemic glucocorticoids could be used in the treatment of severe and refractory abdominal pain, which fail to respond to NSAIDs. Considering kidney manifestations, in children with limited evidence of kidney involvement, only surveillance of urine protein excretion is necessary. When children present with more severe kidney involvement (i.e. proteinuria ≥1 g/day, elevated serum creatinine, or evidence of crescentic glomerulonephritis), immunosuppressive therapy with glucocorticoids is required. Although corticosteroids can provide symptomatic relief, they do not seem to modify the disease course, prevent recurrence or improve prognosis and its usage to prevent kidney or gastrointestinal complications are not indicated.2,6 Moreover, glucocorticoid therapy may elicit usual side effects (e.g: hyperglycemia, hypertension, weight gain, acne and immunosuppression) and additional remarks should be taken into consideration in PHS, which include the risk of masking fever, pain and signs of compromised bowel viability if treatment is started after an intussusception has occurred.6
Additional therapeutic approaches for persistent and recurrent HSP remain controversial and are rarely necessary. However, there are some reports that suggests the use of other immunomodulation agents with promising results. colchicine, dapsone, rituximab, intravenous immune globulin, mycophenolate mofetil, cyclophosphamide and plasmapheresis, especially in cases of aggressive and recurrent disease with kidney involvement, have shown promising results.3,7,8
Considering colchicine and its mechanism of action, some series suggested this drug for the treatment of relapsing HSP.2,3,7 As know, HSP manifests with small vessels inflammation containing neutrophils, which results in fibrinoid necrosis of vessel walls and extravasation of erythrocytes. colchicine is an anti-inflammatory drug, which binds to tubulin and disrupts microtubule assembly, inhibiting neutrophil migration, phagocytic activity and lysosomal degranulation. This drug is effect in gout and familial Mediterranean fever, which are diseases with marked neutrophil accumulation. Interestingly, an increased incidence of HSP with a severe and prolonged course has been reported in association with familial Mediterranean fever.9 The suppressive effect of colchicine on the inflammatory pathway may explain its effect on the skin lesions in HSP.10 Additionally, the use of colchicine allows tapering of corticosteroid therapy, avoiding its potential risks. It can be used safely for at least up to 2 years and some authors affirm that colchicine is less toxic, particularly over the long term than corticosteroids or immunosuppressives. Its usage as also been suggested as first-line treatment, especially in patients with HSP with predominant cutaneous manifestations and lack of systemic involvement.10,11 In our case, colchicine effectively facilitated the tapering of prednisolone, reducing its side effects and preventing recurrences. The temporal correlation between initiating colchicine and gradually reducing corticosteroid therapy, without relapse, strongly supports its beneficial effect in suppressing the inflammatory process.
The potential efficacy of colchicine, coupled with its favorable safety profile, warrants its consideration as a therapeutic choice for severe and chronic HSP in childhood. However, further prospective studies are required to determine the impact of colchicine on the disease progression. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Nelson WE, Behrman RE, Kliegman RW. Nelson Textbook of Pediatrics. 20th ed. Philadelphia: Elsevier; 2016. p. 1216-8.
- Sohagia AB, Gunturu SG, Tong TR, et al. Henoch-schonlein purpura-a case report and review of the literature. Gastroenterol Res Pract. 2010; 2010:597648. doi: 10.1155/2010/597648. [CrossRef] [PubMed] [PMC free article]
- Saulsbury FT. Successful treatment of prolonged Henoch-Schönlein purpura with colchicine. ClinPediatr 2009; 48(8):866-8. doi: 0.1177/0009922809337532. [CrossRef] [PubMed]
- Rigante D, Candelli M, Federico G, et al. Predictive factors of renal involvement or relapsing disease in children with Henoch- Schönlein purpura. Rheumatol Int. 2005; 25:45-48. doi: 10.1007/s00296-004-0452-2 [CrossRef] [PubMed]
- Shin JI, Park JM, Shin YH, et al. Predictive factors for nephritis, relapse, and significant proteinuria in childhood Henoch-Schönlein purpura. Scand J Rheumatol 2006; 35:56-60. doi: 10.1080/03009740510026841 [CrossRef] [PubMed]
- Calvo-Río V, Hernández JL, Ortiz-Sanjuán F, et al. Relapses in patients with Henoch-Schönlein purpura: Analysis of 417 patients from a single center. Medicine (Baltimore) 2016; 95(28):e4217. doi: 10.1097/MD.0000000000004217. [CrossRef] [PubMed] [PMC free article]
- Fotis L, Tuttle PV, Baszis KW, et al. Azathioprine therapy for steroid-resistant Henoch-Schönlein purpura: a report of 6 cases. Pediatr Rheumatol Online J 2016; 23;14(1):37. doi: 10.1186/s12969-016-0100-x. [CrossRef] [PubMed] [PMC free article]
- Jithpratuck W, Elshenawy Y, Saleh H, et al. The clinical implications of adult-onset henoch-schonelin purpura. Clin Mol Allergy 2011; 27;9(1):9. doi: 10.1186/1476-7961-9-9. [CrossRef] [PubMed] [PMC free article]
- Padeh S, Passwell JH. Successful Treatment of Chronic Henoch-Schonlein Purpura with Colchicine and Aspirin. Isr Med Assoc J. 2000; 2(6):482-3.
- Pyne D, Mootoo R, Bhanji A. Colchicine for the treatment of recurrent Henoch-Schönlein purpura in an adult. Rheumatology 2001; 40.12: 1430-1431. doi: 10.1093/rheumatology/40.12.1430. [CrossRef] [PubMed]
- Callen JP. Colchicine is effective in controlling chronic cutaneous leukocytoclastic vasculitis. J Am Acad Dermatol 1985; 13(2Pt 1):193-200. doi: 10.1016/s0190-9622(85)70158-2. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2024.10
|
| Cite this article as: | | Ribeiro J F, Virtuoso J, Pinto A, Oliveira R S, Ferreira J, Salgado M. A Different Approach in a Case of Recurrent Purpura. Pediatr Oncall J. 2024;21: 21-23. doi: 10.7199/ped.oncall.2024.10 |
|