Riddhi Jain, Suneel C Mundkur, Karen Janice Moras, Rochelle Anne Pereira, Divya Mary George.
Department of Paediatrics, Kasturba Medical College, Manipal, Karnataka, India.
ADDRESS FOR CORRESPONDENCE
Dr. Riddhi Jain, Department of Paediatrics, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, 576104, India.
Email: riddhirajeevjain@gmail.com | | Abstract | | First elaborated in 1912 by French physicians Maurice Klippel and Andre Feil, Klippel-Feil syndrome is a congenital condition characterised by faulty segmentation along the embryo’s developmental axis from the 3rd to the 8th week of gestation, resulting in the fusion of two or more cervical vertebrae.1,2 It consists of a clinical triad consisting of a short neck, a limited range of neck motion and a low posterior hairline. However, less than half of the reported cases fulfil the complete triad. There is extensive heterogeneity in presentation involving a wide spectrum of anomalies in the musculoskeletal, central nervous system, auditory, cardiovascular and urogenital System.3 Commonly associated defects include scoliosis, deafness (conductive or sensorineural), mental retardation, Sprengel deformity, renal agenesis and congenital heart defects, the most common being ventricular septal defects.4 Here we present a rare case of Klippel-Feil syndrome with crossed-fused renal ectopia and a large atrial septal defect. | | | | Keywords | | Klippel Feil Syndrome, crossed fused renal ectopia, atrial septal defect. | | | | Case Report | A 6.91-year-old male child presented with a back deformity with the right shoulder blade higher than the left and difficulty abducting the right arm (right Sprengel deformity) noticed since 2 years of age, burning micturition, suprapubic pain and fever since 1 month. The child was a term, AGA baby with a birth weight of 2.5 kg and an uneventful antenatal and neonatal period. The child is developmentally normal, with no delay in attainment of any developmental milestones. The child was born of a non-consanguineous marriage, first in birth order. No family member has a history of similar back deformities.
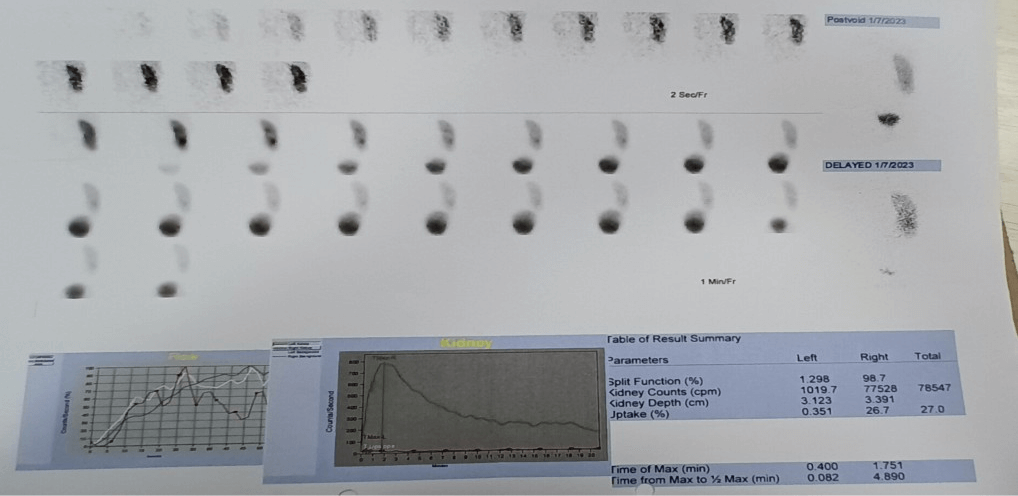
On examination, the child has a short neck (less than 1/13th of total height), a decreased range of neck motion to the left side and a low posterior hairline. The child has a normal stature for his age and physical examination did not reveal any scoliosis, rib or limb anomalies. Blood investigations showed mild iron deficiency anaemia. Urine analysis showed Pyuria and a culture-positive EColi infection. A chest x-ray of the cervical spine showed fusion of the bodies of C2 and C3 vertebrae. USG done showed a single renal mass with two collecting systems visualised in the right renal fossa, suggestive of crossed fused renal ectopia type 3. The echocardiography done showed a large 16X14 mm secondary atrial septal defect with a left-to-right shunt. Tc-99m EC Renogram showed non-visualisation of the left kidney, elongated right kidney, dual pelvic radioactivity and likely left-to-right crossed fused ectopia. Audiological assessment showed bilateral mild conductive hearing loss.
Child was treated with culture-sensitive antibiotics for ongoing urinary tract infection. General paediatrics coordinated among specialties and appropriate referrals were given. Paediatric cardiology advised elective device closure for large ASD and oro-dental hygiene maintenance. Physical and occupational therapy were provided for the improvement of neck range of motion, strength and activities of daily living.
Figure 1. Cervical Xray with fusion of C2 and C3.
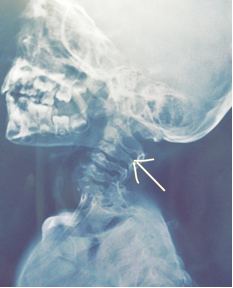
Figure 2. Tc-99m EC Renogram: Left Kidney non visualized. Right kidney is elongated, dual pelvic radioactivity, preserved perfusion and parenchymal radioactive uptake with non obstructive clearance.
Diagnosis:
Klippel-Feil syndrome with large ASD and crossed-fused renal ectopia. | | | | Conclusion | Klippel Feil Syndrome is a rare disorder with an estimated incidence of 0.0025% (1 in 40,000 live births) and a female gender predilection.5,6 Most cases are sporadic. However, autosomal dominant mutations in GDF3, GDF6 (for bone and joint development) and autosomal recessive mutations in genes affecting somatogenesis and vertebral column formation (MEOX1, RIPPLY2) have been identified.7 Treatment is mainly supportive and involves thorough evaluation and management of associated anomalies, requiring multi-disciplinary team involvement. Physiotherapy, activity modification, occupational therapy and oral analgesics also play an important role in improving the overall quality of life. Surgical management is required for patients with poorly controlled pain, upper cervical spine instability, radiculopathy or myelopathy. Caution regarding possible vertebral artery anomalies and difficulty in airway management during surgery needs to be exercised.8
We present a rare case of Klippel Fiel Syndrome with deranged neck movements, symptomatic renal ectopia, bilateral conductive hearing loss, large ASD and not VSD, which is more commonly associated. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Samartzis D, Kalluri P, Herman J, Lubicky JP, Shen FH. "Clinical triad" findings in pediatric Klippel-Feil patients. Scoliosis Spinal Disord. 2016 Jun 27;11:15. doi: 10.1186/s13013-016-0075-x. PMID: 27355085. [CrossRef]
- Frikha R. Klippel-Feil syndrome: a review of the literature. Clin Dysmorphol. 2020 Jan;29(1):35-37. doi: 10.1097/MCD.0000000000000301. PMID: 31577545. [CrossRef]
- Naikmasur VG, Sattur AP, Kirty RN, Thakur AR. Type III Klippel-Feil syndrome: case report and review of associated craniofacial anomalies. Odontology. 2011; 99:197-202. [CrossRef]
- Nagib, M.G., Maxwell, R.E. & Chou, S.N. Klippel-Feil syndrome in children: clinical features and management. Child's Nerv Syst 1, 255-263 (1985). https://doi.org/10.1007/BF00272022. [CrossRef]
- Gruber J, Saleh A, Bakhsh W, Rubery PT, Mesfin A: The prevalence of Klippel-Feil syndrome: A computed tomography-based analysis of 2,917 patients. Spine Deform 2018;6:448-453. [CrossRef]
- Moses JT, Williams DM, Rubery PT, Mesfin A: The prevalence of Klippel-Feil syndrome in pediatric patients: Analysis of 831 CT scans. J Spine Surg 2019;5:66-71. [CrossRef]
- Li Z, Zhao S, Cai S, Zhang Y, Wang L, Niu Y, Li X, Hu J, Chen J, Wang S, Wang H, Liu G, Tian Y, Wu Z, Zhang TJ; DISCO (Deciphering Disorders Involving Scoliosis and COmorbidities) study; Wang Y, Wu N. The mutational burden and oligogenic inheritance in Klippel-Feil syndrome. BMC Musculoskelet Disord. 2020 Apr 11;21(1):220. doi: 10.1186/s12891-020-03229-x. PMID: 32278351; PMCID: PMC7149842. [CrossRef] [PubMed] [PMC free article]
- Litrenta, Jody MD; Bi, Andrew S. MD; Dryer, Joseph W. MD. Klippel-Feil Syndrome: Pathogenesis, Diagnosis, and Management. Journal of the American Academy of Orthopaedic Surgeons 29(22):p 951-960, November 15, 2021. | DOI: 10.5435/JAAOS-D-21-00190. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2024.60
|
| Cite this article as: | | Jain R, Mundkur S C, Moras K J, Pereira R A, George D M. Rare Manifestation of Klippel Feil Syndrome with Crossed Fused Renal Ectopia and Atrial Septal Defect. Pediatr Oncall J. 2024;21: 163-164. doi: 10.7199/ped.oncall.2024.60 |
|