Catarina Macedo Francisco1, Pedro Pereira2, Íris Santos Silva1, Pedro Fernandes1, António P. Pissarra3.
1Pediatrics Department, Hospital Sousa Martins, Guarda, Portugal,
2General surgery Department, Hospital Sousa Martins, Guarda, Portugal,
3Medical Imaging Department, Hospital Sousa Martins, Guarda, Portugal.
ADDRESS FOR CORRESPONDENCE
Catarina Macedo Francisco, Rua José Afonso, nº7, 2º direito, 1600-130, Lisboa.
Email: catarinamfrancisc@gmail.com | | Abstract | Abdominal pain is one of the most common causes of Hospital admission;
nevertheless, a thorough investigation should always be performed.
We present the case report of a 14-year-old girl, institutionalized and with history of Psychiatric disease, admitted to the Emergency Department (ED) due to intense abdominal pain in the context of obstipation, a condition already known in this patient.
Due to worsening of her complaints, she was hospitalized and the final diagnostic was only possible with the collaboration between different specialties – Pediatrics, Radiology and General Surgery.
The etiology revealed to be quite serious and so adequate treatment was rapidly performed. | | | | Keywords | | pediatrics, bezoar, adolescence, trichobezoar. | | | | Introduction | Abdominal symptoms are among the most common reasons for pediatric emergency department visits and abdominal pain is the most frequently reported symptom. When physicians are facing a patient with this complaint, thorough history taking and physical examination can often reach the correct diagnosis.1
In some cases, however, imaging tests are indicated, such as ultrasound or plain-film x-ray studies. Computed Tomography (CT) is reserved for specific indications and in individual cases, for example, in patients with high clinical suspicion of abdominal disease and inconclusive findings at ultrasonography.1 | | | | Case Report | The authors present the case of a 14-year-old female, institutionalized and with history of psychiatric disorder, admitted to the Emergency Department (ED) due to severe abdominal cramps.
The patient referred a constant and intense pain, without any relief factor, with periods of exacerbation that were not always related to meals. The pain was located in the upper left quadrant, with no radiation.
The patient had these complaints for several months and associated this pain with chronic obstipation (previously diagnosed) and which had already caused several visits to the ED (the last one the day before due to the same symptoms). The patient gave a history of passing hard stools and had irregular bowel movements, the last of which was about 3 days ago.
The patient denied fever, nausea or vomiting, although there was an episode of the latter after admission to the ED.
Regarding medical background, this patient was institutionalized and was being followed by the Child Psychiatry Department, previously diagnosed with depression and taking risperidone 0.5 mg once a day.
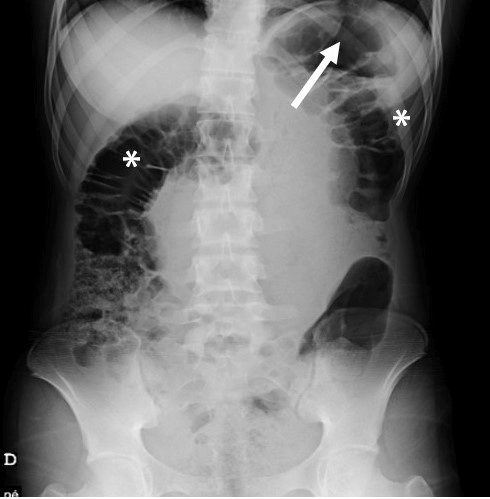
On physical examination, the patient was pale and had diffuse and intense tenderness on abdominal palpation. An abdominal X-ray, that depicted gastric distension, with a high air fluid level. Air-filled colonic distention was also evident (Figure 1).
Figure 1. Supine AP plain film X-ray upon admission, showing gastric (arrow) and colonic (asterisks) distension.
After the bowel enema, the pain persisted and the patient was then hospitalized, in order to perform treatment for fecal impaction.
Her blood tests were performed: Hb: 10 g/dL; MCV: 74.7 fL; MCH: 20.9 pg; MCHC:27.9 g/dL; RDW: 16.9%; Platelets: 534 10^3/μL; Total proteins: 5.18 g/dL; albumin: 3.17 g/dL; Ferritin: 2.3 ng/ml.
There was worsening of the patient condition, with pain progressively more intense. On the second day of hospitalization, an abdominal ultrasound was requested, which was particularly impaired due to intense diffuse bowel gas interposition but that depicted the presence of free intraperitoneal fluid. Taking that into consideration and adding to the patient’s general condition, an abdominal and pelvic CT scan was performed.
The CT scan confirmed the presence of intraperitoneal free fluid, with associated abnormal peritoneal enhancement, in keeping with peritonitis. Besides that, there was marked gastric distension filled by a heterogeneous mass up to the pylorus and free intraperitoneal air was also present (Figure 2). These findings raised the suspicion of a trichobezoar complicated with gastric perforation and an emergent median supra umbilical laparotomy was then performed (Figure 3). There was also presence of left pleural effusion.
Figure 2. CT-scan showing a voluminous and well-defined trichobezoar (asterisks) and free intraperitoneal air (arrows). Left pleural effusion was also present.
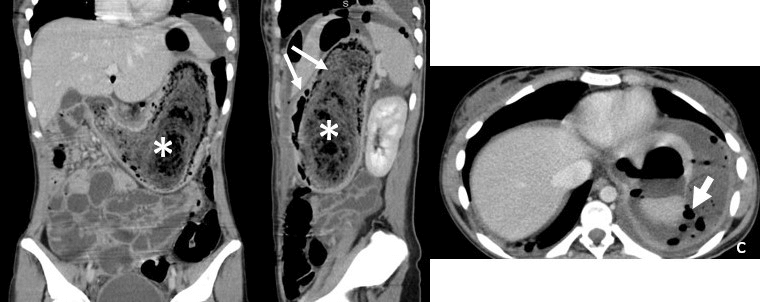
Figure 3. Surgical removal of the trichobezoar.

Gastrostomy was performed, with extraction of a voluminous trichobezoar from the patient’s stomach, of about 20 cm long (Figure 4). The patient had already considerable gastric distension, with perforation of the antrum and chemical peritonitis.
Figure 4. Trichobezoar, 20 cm long.

After extraction, several complications developed, with worsening of her microcytic hypochromic anemia (Hb: 7.7 g/dl, MCV 72.2 fL, MCHC 29.4 g/dl) and transfusion of 1 unit of packed red blood cells was needed. The patient also developed hypoproteinemia and hypoalbuminemia, with consequent increase of the pleural effusion already present and due to this she received albumin (1 g/kg/ev). Nonetheless, her bowel movement was completely restored.
After surgery, a second and more thorough clinical history was performed and the patient admitted having frequent episodes of trichophagia, as part of her underlying psychiatric condition.
After contacting the Child Psychiatry Department while the patient was hospitalized, the risperidone dose was doubled to 1 mg once daily. She was then transferred to a tertiary hospital, in order to drain the pleural effusion.
Currently, she is followed in Pediatric consultation and maintains some respiratory complaints due to the presence of residual pleural effusion.
She maintains aggressive behaviors, with auto-mutilation episodes and is now being medicated with risperidone, escitalopram and quetiapine.
The GIT movement was completely restored and she fully recovered from her anemia, although she had to take oral iron supplements for 3 months.
| | | | Discussion | A bezoar is defined as a mass of undigested material that accumulates in the gastrointestinal tract (GIT) and is usually located in the stomach. It’s a rare condition (making up to 0.3% of upper tract endoscopies2) and usually is an incidental finding.
It can consist of food (mainly fibrous components from fruits or vegetables), ingested medication, foreign bodies (such as tissue paper, shellac, foams…etc.) or human hair (the latter defined as a trichobezoar).3 Their incidence is higher in adolescents and in females and is usually associated to psychiatric or cognitive dysfunction.4
Gastric bezoars can cause unspecific symptoms, such as abdominal distension, pain, nausea, vomiting or anorexia and can be a true diagnostic challenge, as they can remain asymptomatic for many years.5 Once they reach considerable dimensions, gastric bezoars can cause obstruction and hence, intestinal occlusion. The most common complications described in the literature are gastric perforation, protein losing enteropathy, steatorrhea, pancreatitis, appendicitis, jaundice or intestinal intussusception.4
In this particular case, the failure of response after faecal disimpaction with persistence of constant pain, was a sign that the cause couldn’t only be functional. This led to the realization of more specific exams, that confirmed the diagnosis and urgent treatment was possible, avoiding potential more serious complications.
Regarding the treatment, there are several possibilities, such as chemical dissolution (cellulase, acetylcysteine), endoscopic removal, prokinetics administration (metoclopramide) or surgical removal.6
In the case presented, surgical approach was the more appropriate for the patient, since she had a perforation suspicion, which was confirmed during surgery.
With this clinical case, we can conclude that among adolescents, the prevalence of psychosomatic symptomatology is common and there is a tendency to amplify symptoms, which can lead healthcare professionals to relate these symptoms with a psychologic etiology.
Nevertheless and as described in this clinical case, sometimes the cause can be serious if left untreated. The patient’s overall state was an important indicator of the severity of the condition. This is important, especially in patients with psychiatric or cognitive disturbances, in which these symptoms can be easily overlooked.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- D.Coca RobinotC.Liébana de RojasE.Aguirre Pascual, Abdominal emergencies in paediatrics, Radiologia, 2016 May;58 Suppl 2:80-91. [CrossRef]
- C H Andrus 1, J L Ponsky, Bezoars: classification, pathophysiology, and treatment, Am J Gastroenterol, 1988 May.
- Kadian RS, Rose JF, Mann NS. Gastric bezoars--spontaneous resolution. Am J Gastroenterol 1978; 70:79. [CrossRef]
- DeBakey M, Oshner A. Bezoars and concretions. Surgery 1938; 4:934.
- Prisant LM, Carr AA, Bottini PB, Kaesemeyer WH. Nifedipine GITS (gastrointestinal therapeutic system) bezoar. Arch Intern Med 1991; 151:1868. [CrossRef]
- Iwamuro M, Okada H, Matsueda K, Inaba T, Kusumoto C, Imagawa A, Yamamoto K. Review of the diagnosis and management of gastrointestinal bezoars. World J Gastrointest Endosc 2015; 7(4): 336-345. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2025.62
|
| Cite this article as: | | Francisco C M, Pereira P, Silva Í S, Fernandes P, Pissarra A P. Trichobezoar: the importance of a multidisciplinary approach. Pediatr Oncall J. 2025;22. doi: 10.7199/ped.oncall.2025.62 |
|