Benjamin Wei-Liang Ng1, Jeffrey Soon-Yit Lee2, Teck-Hock Toh1,2.
1Department of Pediatrics, Sibu Hospital, Ministry of Health Malaysia, Sibu, Sarawak, Malaysia,
2Clinical Research Centre, Sibu Hospital, Ministry of Health Malaysia, Sibu, Sarawak, Malaysia.
ADDRESS FOR CORRESPONDENCE
Dr Benjamin Wei-Liang Ng, Department of Pediatrics, Sibu Hospital, Jalan Ulu Oya, 96000 Sibu, Sarawak, Malaysia.
Email: benng85@gmail.com | | Abstract | | Moyamoya vasculopathy (MMV) is a rare progressive stenosis of the intracranial internal carotid arteries (ICA) and its branches with characteristic collateral formation. MMV frequently manifests in children as ischemic stroke or transient ischemic attack (TIA). The recognition of TIA in a child with MMV can be challenging due to the overlapping features seen with stroke-mimics, causing missed or delayed diagnosis. Ischemic symptoms seen in MMV are often triggered by hyperventilation, crying or exercise, but the association with spicy food is rare. We describe a boy with recurrent episodes of TIA associated with eating spicy food. After several misdiagnoses, a thorough re-evaluation and a magnetic resonance angiographic imaging confirmed the diagnosis of MMV. Neurosurgical revascularization surgery was performed with good post-operative outcome on follow-up. This case highlights the unusual association of spicy food and TIA in a child with MMV and illustrates the conundrum surrounding its diagnosis. | | | | Keywords | | Moyamoya vasculopathy, transient ischemic attack, spicy food. | | | | Introduction | Moyamoya vasculopathy (MMV) is a rare intracranial arteriopathy characterized by chronic progressive cerebrovascular steno-occlusive changes seen over the terminal internal carotid artery (ICA), middle cerebral artery (MCA) and/or proximal anterior cerebral artery (ACA) with simultaneous formation of prominent arterial collateral vessels.1,2 The term ‘moyamoya’ is coined to represent the distinctive angiographic finding of dilated collateral arteries which resemble ‘a puff of smoke in the air’ seen in the base of the brain associated with this disorder.1,2
Moyamoya vasculopathy accounts for 6-10% of childhood strokes and TIA.2,3 The incidence is higher in East Asian countries such as Japan, Korea and China.4 Cases were also documented in Europe and the United States, albeit less often.4 The term MMV is used to describe both the idiopathic variant, known as moyamoya disease (MMD) and moyamoya syndrome (MMS) which represents the subgroup associated with other conditions such as Down syndrome, neurofibromatosis, meningitis or vasculitis.4,5,6,7 There is increasing recognition for the role of genetics as a predisposing factor in those previously classified as MMD, specifically involving the mutations of RNF213 gene.5
Most children with MMV present with ischemic strokes or TIA.7,8,9 Headache, seizures and involuntary movements have also been reported. Cerebral hemorrhage due to MMV is rare in children compared to adults.2,4 A large majority reported paralysis or weakness of the extremities precipitated by crying, hyperventilation, blowing or coughing.10 The association of these ischemic symptoms with spicy food consumption is rare and the mechanism is not well understood. We describe a boy with recurrent transient right-sided body weakness peculiarly brought on by consuming spicy food, leading to an initial diagnostic conundrum. His imaging study later revealed left ICA occlusive changes with moyamoya collaterals. This case report aims to illustrate the unusual association of spicy food and TIA in a child with MMV and the challenges surrounding the diagnosis, highlighting the need for careful evaluation of the clinical and radiological findings.
| | | | Case Report | An eight-year-old Chinese boy presented with recurrent right upper limb weakness for three years. The first episode was reported at five years of age while eating spicy noodles. He reported numbness over the right upper limb, which progressed rapidly to weakness. There was no altered awareness and no abnormal movement or posture. The weakness lasted for less than three minutes with a complete regain of function, but the numbness lasted for half an hour. In the first two years, these episodes recurred three to four times a year, mostly associated with spicy food consumption.
The family did not seek medical advice initially as the episodes were self-limiting without residual neurological deficits. Over time, these episodes became more frequent, occurring once every fortnight to monthly and eventually started to involve the right face and lower limb. These symptoms were occasionally precipitated by vigorous crying or tantrums, unrelated to spicy food consumption. During one of the recent episodes, he became disorientated with slurred speech, prompting an outpatient consultation with a pediatrician. The parents were reassured that their child was well because the examination was normal and the symptoms had completely resolved. This reaffirmed the family’s belief that these episodes were behavioral in nature.
Nevertheless, the family sought a second opinion at our hospital as his symptoms became even more frequent. A video recording of one of the earlier episodes was reviewed, showing him sitting down while eating his spicy noodle but with facial asymmetry and unable to lift his right upper limb while the left arm was reaching out for his food. In the clinic, neurological examination showed normal tone, power and reflexes in all limbs. Cranial nerves were normal and there were no neurocutaneous lesions or dysmorphisms. His blood pressure and echocardiogram were unremarkable. There was no family history of seizures or young stroke. He was an average student in school with no reported decline in academic performance or change in behavior.
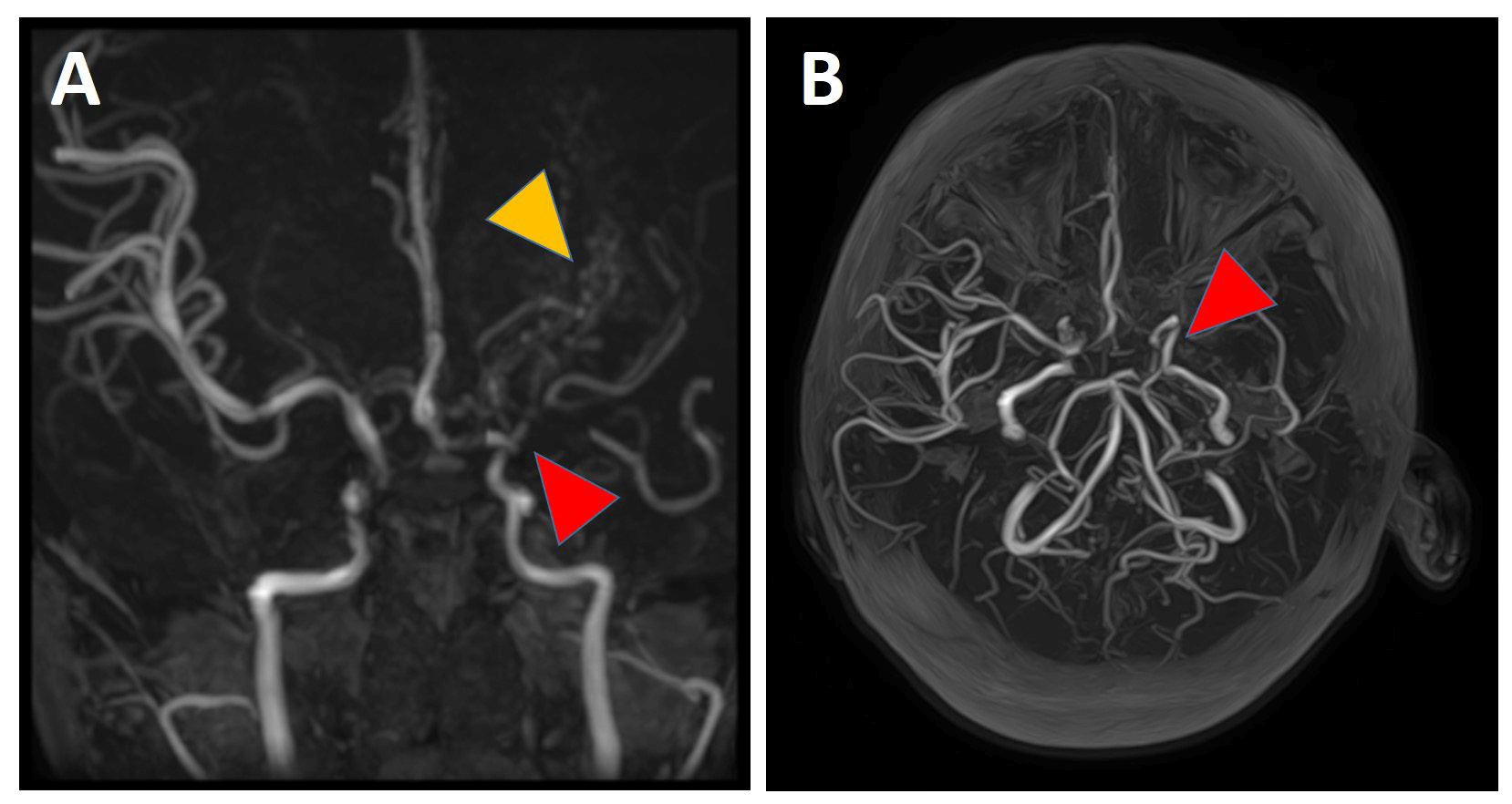
The initial evaluation led to the preliminary diagnosis of a focal seizure. Magnetic resonance imaging (MRI) of the brain and electroencephalogram (EEG) were normal. Subsequently, re-evaluation of more recent recordings revealed a hemiplegic gait on top of the earlier signs, suggesting an acute ischemic event. A magnetic resonance angiography (MRA) showed stenosis at the left ICA extending to the ACA and the entire length of the MCA with multiple small collateral vessels, consistent with moyamoya vasculopathy. (Figure 1) A diagnostic digital subtraction angiography (DSA) later confirmed the MRA findings with collaterals seen at the left basal ganglia and perfusion defect at the left parietal region, consistent with Suzuki Stage III disease.
Figure 1. (A) The MRA shows narrowing at the supraclinoid portion of the left ICA (red arrow) extending to the A1 of the left ACA and MCA entirely, with generalized reduced vasculature of the left cerebral hemisphere. Multiple collateral vessels, resembling ‘a puff of smoke’ are seen in this region (yellow arrow). The rest of the left ACA is patent and of normal caliber.
(B) Three-dimension reconstruction of the MRA imaging shows stenosis at the intracranial portion of the ICA with subsequent reduced vasculature beyond this point (red arrow).
Management and Outcome
The child was started on 3 mg/kg/dose of oral aspirin daily and subsequently referred to the neurosurgeons in a tertiary hospital for revascularization surgery. He underwent encephaloduroarteriosynangiosis (EDAS), an indirect cerebral revascularization procedure two months after the diagnosis with success and uneventful post-operative recovery. (Figure 2) Three months post-operatively, his symptoms improved with lesser frequency and severity. He is planned for a repeat scan in six months to re-evaluate the formation of collateral vasculature post-procedure.
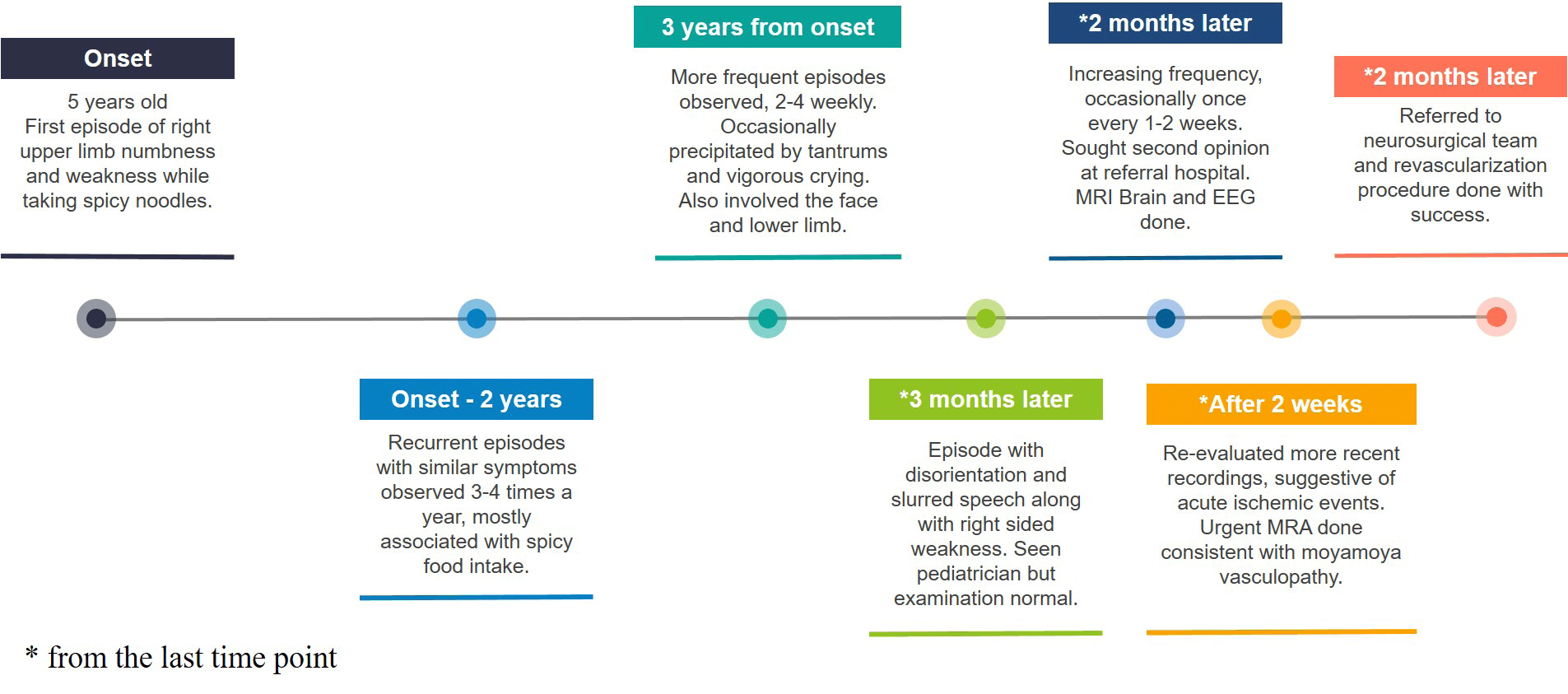
Figure 2. Timeline shows the chronology of events over three years from the onset of the symptoms to the diagnosis of MMV and subsequent intervention.
| | | | Discussion | The clinical presentation of MMV is variable depending on the expression of the disease and the age of presentation. According to the International Pediatric Stroke Study, 90% of children with MMV presented initially with ischemic stroke and another 7.5% with TIA.8 TIA in adults has been extensively researched due to a growing recognition of the subsequent elevated risk of developing a major cerebrovascular accident within three months of presentation.11 On the contrary, there is a dearth of data on childhood TIA as it is less common compared to other mimics such as focal seizure, post-ictal Todd’s paresis, complicated migraine or functional neurological disorders. The clinical features of TIA may overlap with other stroke-mimics, resulting in missed or delayed diagnosis.12 Thus, recognizing TIA in children is challenging and requires a high index of suspicion and experience.
This case posed a similar diagnostic conundrum because the TIA symptoms exhibited are similar to those of other diseases. Table 1 lists some of the differential diagnoses to consider and the features to better discriminate these conditions when the initial MRI brain is normal.
Table 1. Differential diagnosis for transient recurrent unilateral weakness with normal MRI brain imaging.
| |
Points for |
Points against |
| Focal onset seizure |
- Frequently involves only one side of the body.
- Short duration of symptom with complete neurological recovery.
- May be associated with disorientation/confusion
|
- More commonly associated with positive* motor symptoms such as unilateral limb jerking/clonic movement, only very rarely associated with paresis from the onset.13
- Lack of pre-ictal auras which are commonly associated with focal seizures.
- Lack of post-ictal events.
- May be associated with a unilateral intracranial lesion which can be detected on imaging.
|
| Functional neurologic disorder |
- Association with emotional stressor (tantrum and vigorous crying).
- Atypical association of onset of weakness with spicy food intake.
|
- Unilateral weakness involving the face, upper and lower limbs, which is consistent with a specific vascular territory.14
- Fairly consistent clinical presentation during each episode.
- Difficult to voluntarily execute the complex motor signs to mimic the precise anatomic distribution.
|
| Functional neurologic disorder |
- Symptoms occurred abruptly with a gradual offset13, over minutes.
- Negativel symptoms from onset - unilateral limb weakness, affecting face and mobility.
- Intact awareness.
- Recurring over days to weeks.
- Short duration of symptom with complete neurological recovery.
|
- Less common cause of unilateral weakness in children, unless with predisposing cerebrovascular anomalies.
|
| Complicated migraine |
- Manifestation of negative symptoms – numbness progressing to weakness over the same body site distribution.
- Intact awareness.
|
- Progresses slowly over minutes, less abrupt and may last for many hours.
- Lack of headache or visual symptoms described in the presentation.
|
* Positive symptoms - representing an excess of central nervous system electrical discharges affecting visual, somatosensory or motor components.
l Negative symptoms - representing a loss of central nervous system function such as visual or hearing loss, reduced sensation or power in the limbs.
Several studies identified some characteristics that differentiate TIA from other mimics in children. This is imperative to reduce the diagnostic delay and allow prompt intervention to minimize the risk of catastrophic cerebrovascular events. Mackay et al. proposed that stroke is more likely if a child is well a week before presentation, is unable to walk or has focal facial or arm weakness.15 Conversely, vomiting, visual and sensory disturbances and the absence of focal signs are less likely to represent a cerebral ischemic event. Unlike adults, seizures are not uncommon in childhood stroke and are reported in 30% of cases.8 Therefore, the diagnosis of seizure does not completely exclude an ischemic event in children, particularly if the ‘seizure’ has an atypical semiology like focal atonic or with predominantly negative symptoms.12,16 In such recurrent ‘seizure’ episodes, more extensive investigations including cerebral vascular imaging should be considered early to rule out ischemic events. Our patient was initially misdiagnosed with a focal seizure. However, in hindsight, the predominantly negative symptoms with unilateral facial and limb weakness were more consistent with TIA.
One of the other differential diagnoses considered in our case was functional disorder or behavioral issues. Dooley et al. described the approach to differentiate functional from organic conditions based on history and examination, but this remained challenging in our daily clinical practice.17 In our case, the brief episodes, normal physical examination, temporal association with emotional distress, the peculiar association with spicy food consumption and a normal MRI brain overall favors a functional rather than an organic disorder. However, the signs manifested were anatomically consistent with a vascular domain. In retrospect, it is highly doubtful that the child could voluntarily execute such complex neurological symptoms. More importantly, as demonstrated in our case, a normal brain MRI alone does not exclude organic causes. Careful reassessment of the history and physical examination is crucial especially when there is incongruence between the radiological and clinical findings. Therefore, such an unusual presentation should be approached cautiously to elicit an organic explanation.
Several mechanisms were postulated to explain the effects of spicy food on cerebral vessels.18 Spicy food can cause hyperventilation which triggers hypocapnia-induced cerebral vasoconstriction.18,19 However, in our case, prior episodes of hyperventilation from physical activities or crying had never triggered any symptoms until the recent association with spicy food. Thus, there may be other compounding mechanisms that augment the vasoconstrictive effect. capsaicin, a vasoactive compound found in chilies is known for its cardioprotective properties. One of these beneficial effects includes modulation of the coronary blood flow via the activation of transient receptor potential channels, which induces an endothelium-dependent vasodilation through stimulation of endothelial nitric oxide synthase.20,21
However, several study findings suggest that high concentrations of capsaicin can induce coronary vasospasm and myocardial ischemia. An animal study by Szolcsanyi et al. demonstrated that capsaicin causes a concentration-dependent constriction of the coronary arteries and reduces the blood flow via its effect on the Vanilloid Receptor1 (VR1).22Edvinsson et al. observed a similar concentration-dependent vasoconstrictive effect in the cerebral vasculature,23which may be explained by the effect of capsaicin on the VR1 receptors found in cerebral vessels. Several reported cases of reversible cerebral vasoconstriction syndrome caused by excessive consumption of capsaicin further support this association.24,25,26 Furthermore, the notion of ‘excess’ may be relative; an equal serving of spicy food may contain a tolerable amount of capsaicin for an adult but excessive for a child. Therefore, the precipitation of the initial symptoms in our case is likely caused by augmented vasoconstriction from the combined effects of hyperventilation and the relative capsaicin excess.
MMV is a progressive intracranial vasculopathy with no curative treatment to date. Suzuki et al. categorized the progression of the moyamoya vessels into six stages, beginning with just narrowing of the ICA bifurcation in stage I to the complete disappearance of the moyamoya collaterals and ICA vessel system in stage VI.27Surgical revascularization may be offered to those with recurrent ischemic symptoms or asymptomatic but with impaired cerebral hemodynamic, with the aims of reducing the risk of complications and morbidity.28Our patient’s symptoms were initially primarily triggered by spicy food, but gradually became more readily precipitated by other factors like crying or tantrums. This signified the progression of his disease with a pre-procedure DSA showing Suzuki stage III disease with perfusion defect, which warranted an early intervention. Surgical options include the direct technique and indirect techniques. Studies have shown better long-term outcomes in those with surgical revascularization versus those managed conservatively, in terms of risk of subsequent stroke.29,30 Additionally, a systematic review reported symptomatic improvement in 87% of cases post-operatively.31 Therefore, prompt diagnosis is pertinent to enable early evaluation for surgical intervention or to institute early imaging surveillance with medical therapy.
In conclusion, the overlapping symptoms between TIA and the mimics makes the diagnosis of MMV challenging. A thorough history and recognition of hemiparesis in a child should prompt clinicians to consider early cerebral vascular imaging. Future research should elucidate the exact pathophysiological mechanisms of cerebrovascular events precipitated by spicy food.
Learning Points:
1. TIA is a common manifestation in children with MMV, but the diagnosis can often be misled by the overlapping features of other stroke- or TIA-mimics.
2. Spicy food, though a rare association, may be a possible trigger for cerebral ischemic event via mechanisms such as hyperventilation-induced vasoconstriction and the vasoactive effect of capsaicin on cerebral vasculatures.
3. In children presenting with recurrent unilateral limb weakness and facial involvement, cerebral vascular imaging should be considered even with an initial normal brain imaging.
4. Early recognition of TIA caused by MMV is imperative to plan for early surgical intervention and reduce the risk of stroke and morbidity.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Zhang A, Brown N, Cheaney B, et al. Updates in the management of moyamoya disease; Interdisciplinary Neurosurgery, Volume 23, 2021,100976, ISSN 2214-7519, https://doi.org/10.1016/j.inat.2020.100976. [CrossRef]
- Smith JL. Understanding and treating moyamoya disease in children. Neurosurg Focus. 2009 Apr;26(4):E4. doi: 10.3171/2000.01.FOCUS08306. PMID: 19335128. [CrossRef]
- Po' C, Nosadini M, Zedde M, et al. Pediatric moyamoya disease and syndrome in Italy: A multicenter cohort. Front Pediatr. 2022 May 6;10:892445. doi:10.3389/fped.2022.892445. PMID: 35601411; PMCID: PMC9120837. [CrossRef]
- Lim WK, Ong LC, Tan KA, et al. Clinical features and outcomes of paediatric moyamoya vasculopathy in Malaysia; Neurology Asia 2022; 27(3):617 - 627. doi: https://doi.org/10.54029/2022pvt [CrossRef]
- Pilgram-Pastor S, Chapot R, Kraemer M. The angiographic presentation of European moyamoya angiopathy. J Neurol. 2022 Feb;269(2):997-1006. doi: 10.1007/s00415-021-10684-6. [CrossRef]
- Kuroda S, Fujimura M, Takahashi J, et al. Research Committee on moyamoya disease (spontaneous occlusion of Circle of Willis) of the Ministry of Health, Labor, and Welfare, Japan. Diagnostic criteria for moyamoya disease - 2021 Revised Version. Neurol Med Chir (Tokyo). 2022 Jul 15;62(7):307-312. doi: 10.2176/jns-nmc.2022-0072. [CrossRef]
- Toh, T. H., Siew, E. C., Chieng, C. H., & Mohd Ismail, H. I. Post intravenous immunoglobulin stroke in a toddler with Down syndrome: a diagnostic challenge. BMJ Case Reports. 2020;13(5), e233149. https://doi.org/10.1136/bcr-2019-233149. [CrossRef]
- Lee S, Rivkin MJ, Kirton A, et al. Moyamoya disease in children: Results from the International Pediatric Stroke Study; International Pediatric Stroke Study; J Child Neurol. 2017; 32(11):924. Epub 2017 Jul 17. [CrossRef]
- Ferriero DM, Fullerton HJ, Bernard TJ, et al. American Heart Association Stroke Council and Council on Cardiovascular and Stroke Nursing. Management of stroke in neonates and children: A scientific statement from the American Heart Association/American Stroke Association. Stroke. 2019 Mar;50(3):e51-e96. doi: 10.1161/STR.0000000000000183. PMID: 30686119. [CrossRef]
- Amlie-Lefond C, Ellenbogen RG. Factors associated with the presentation of moyamoya in childhood. J Stroke Cerebrovasc Dis. 2015 Jun;24(6):1204-10. doi: 10.1016/j.jstrokecerebrovasdis.2015.01.018. Epub 2015 Apr 10. PMID: 25866319. [CrossRef]
- Hill MD, Coutts SB. Preventing stroke after transient ischemic attack. CMAJ. 2011 Jul 12;183(10):1127-8. doi: 10.1503/cmaj.110704. Epub 2011 Jun 6. PMID: 21646467; PMCID: PMC3134717. [CrossRef]
- Fitzsimons BT, Fitzsimons LL, Sun LR. Laney's story: The problem of delayed diagnosis of pediatric stroke. Pediatrics. 2019 Apr;143(4):e20183458. doi: 10.1542/peds.2018-3458. Epub 2019 Mar 12. PMID: 30862727. [CrossRef]
- Nadarajan V, Perry RJ, Johnson J, et al. Transient ischaemic attacks: mimics and chameleons. Pract Neurol. 2014 Feb;14(1):23-31. doi: 10.1136/practneurol-2013-000782. PMID: 24453269; PMCID: PMC3913122. [CrossRef]
- Cucchiara B, Kasner SE. In the clinic. Transient ischemic attack. Ann Intern Med. 2011 Jan 4;154(1):ITC11-15; quiz ITC1-16. doi: 10.7326/0003-4819-154-1-201101040-01001. PMID: 21200033. [CrossRef]
- Mackay MT, Lee M, Yock-Corrales A, et al. Differentiating arterial ischaemic stroke from migraine in the paediatric emergency department. Dev Med Child Neurol. 2018 Nov;60(11):1117-1122. doi: 10.1111/dmcn.13772. Epub 2018 Apr 14. PMID: 29655223. [CrossRef]
- Park JT, Fernandez-Baca Vaca G. Epileptic seizure semiology in infants and children. Seizure. 2020 Apr;77:3-6. doi: 10.1016/j.seizure.2019.10.015. Epub 2019 Oct 24. PMID: 31708348. [CrossRef]
- Dooley JM, Gordon KE. Spurious neurological signs and symptoms in children. Paediatr Child Health. 2011 Aug;16(7):e51-3. doi: 10.1093/pch/16.7.e51. PMID: 22851901; PMCID: PMC3200379. [CrossRef]
- Dubey S, Ghosh R, Chatterjee S, et al. Spicy foods triggering clinical symptoms in moyamoya angiopathy. J Neurosurg Sci. 2021 Feb;65(1):85-88. doi: 10.23736/S0390-5616.20.05030-4. Epub 2020 Jun 17. PMID: 32550609. [CrossRef]
- Mathew T, Souza DD, John SK, et al. Transient ischemic attack after eating spicy foods in children: Think of moyamoya disease. Neurol India. 2021 Jul-Aug;69(4):1032-1033. doi: 10.4103/0028-3886.325347. PMID: 34507437. [CrossRef]
- Guarini G, Ohanyan VA, Kmetz JG, et al. Disruption of TRPV1-mediated coupling of coronary blood flow to cardiac metabolism in diabetic mice: role of nitric oxide and BK channels. Am J Physiol Heart Circ Physiol. 2012 Jul 15;303(2):H216-23. doi: 10.1152/ajpheart.00011.2012. Epub 2012 May 18. PMID: 22610171. [CrossRef]
- McCarty MF, DiNicolantonio JJ, O'Keefe JH. Capsaicin may have important potential for promoting vascular and metabolic health. Open Heart. 2015 Jun 17;2(1):e000262. doi: 10.1136/openhrt-2015-000262. PMID: 26113985; PMCID: PMC4477151. [CrossRef]
- Szolcsanyi J, Oroszi G, Nemeth J, et al. Functional and biochemical evidence for capsaicin-induced neural endothelin release in isolated working rat heart. Eur J Pharmacol 2001;419(23):215-221. [CrossRef]
- Edvinsson L, Jansen I, Kingman TA, et al. Cerebrovascular responses to capsaicin in vitro and in situ. Br J Pharmacol. 1990 Jun;100(2):312-8. doi: 10.1111/j.1476-5381.1990.tb15801.x. PMID: 2379036; PMCID: PMC1917408. [CrossRef]
- Thottempudi N, Kovalev D, Munder SP, et al. Reversible cerebral vasoconstriction syndrome following exposure to Oleoresin Capsicum "Pepper Spray". J Stroke Cerebrovasc Dis. 2021 Oct;30(10):106006. doi: 10.1016/j.jstrokecerebrovasdis.2021.106006. Epub 2021 Jul 26. PMID: 34325271. [CrossRef]
- Taylor CS, Kelly BM, Nichols TA. Fear the reaper: reversible cerebrovascular vasoconstriction syndrome after hot pepper ingestion. Radiol Case Rep. 2020 Apr 5;15(6):641-643. doi: 10.1016/j.radcr.2020.02.025. PMID: 32280392; PMCID: PMC7136587. [CrossRef]
- Suzuki J, Takaku A. Cerebrovascular "moyamoya" disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol. 1969 Mar;20(3):288-99. doi: 10.1001/archneur.1969.00480090076012. PMID: 5775283. [CrossRef]
- Boddhula SK, Boddhula S, Gunasekaran K, et al. An unusual cause of thunderclap headache after eating the hottest pepper in the world - "The Carolina Reaper". BMJ Case Rep. 2018 Apr 9;2018:bcr2017224085. doi: 10.1136/bcr-2017-224085. PMID: 29632122; PMCID: PMC5893965. [CrossRef]
- Acker G, Fekonja L, Vajkoczy P. Surgical management of moyamoya disease. Stroke. 2018 Feb;49(2):476-482. doi: 10.1161/STROKEAHA.117.018563. Epub 2018 Jan 17. Erratum in: Stroke. 2018 Mar;49(3):e143. PMID: 29343587. [CrossRef]
- Wouters A, Smets I, Van den Noortgate W, et al. Cerebrovascular events after surgery versus conservative therapy for moyamoya disease: a meta-analysis. Acta Neurol Belg. 2019 Sep;119(3):305-313. doi: 10.1007/s13760-019-01165-9. Epub 2019 Jun 18. PMID: 31215004. [CrossRef]
- Li Q, Gao Y, Xin W, et al. Meta-Analysis of prognosis of different treatments for symptomatic moyamoya disease. World Neurosurg. 2019 Jul;127:354-361. doi: 10.1016/j.wneu.2019.04.062. Epub 2019 Apr 14. PMID: 30995556. [CrossRef]
- Fung LW, Thompson D, Ganesan V. Revascularisation surgery for paediatric moyamoya: a review of the literature. Childs Nerv Syst. 2005 May;21(5):358-64. doi: 10.1007/s00381-004-1118-9. Epub 2005 Feb 5. PMID: 15696334. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2025.63
|
| Cite this article as: | | Ng B W, Lee J S, Toh T. Spicy food induced transient ischemic attack: A diagnostic conundrum in a child with moyamoya vasculopathy.. Pediatr Oncall J. 2025;22. doi: 10.7199/ped.oncall.2025.63 |
|