Karen Janice Moras, Suneel C Mundkur, Rochelle Anne Periera.
Department of Pediatrics, Kasturba Medical College, MAHE, Manipal University, Manipal, India.
ADDRESS FOR CORRESPONDENCE
Karen Janice Moras, Associate Professor, Department of Pediatrics, Kasturba Medical College, MAHE, Manipal University, Manipal-576104, India.
Email: drkarenmoras87@gmail.com | | Abstract | | Hepatic involvement in COVID-19 in children is typically characterized by elevation in Alanine transaminase (ALT) and Aspartate aminotransferase (AST) with preserved liver synthetic function.1 Severe hepatic involvement in COVID-19 is seen in COVID Multisystem Inflammatory Syndrome in Children (MIS-C), which typically occurs several weeks to months after the initial SARS-CoV-2 infection rather than during acute infection.2, 3 However, there is a paucity of literature describing Paediatric cases of cholestatic jaundice as a primary manifestation of acute SARS-CoV-2 infection. We report two cases of cholestatic jaundice as the primary manifestation of COVID-19. | | | | Keywords | | Pediatric COVID-19, cholestasis, jaundice, SARS-CoV-2 infection. | | | | Case Report | Case 1
An 8 year old male child presented with fever since one week, with generalised urticaria. The rash started in the trunk progressed to involve the upper limbs and lower limbs and face. Eyes showed conjunctival congestion. Genitalia and oral cavity were normal. No history of rhinitis, cough, difficulty in breathing. No history of allergy, atopy. No history of travel or drug intake. Growth and development were normal. His vaccination was age appropriate. On day 3 of admission, he developed jaundice with itching. There was no past history or family history of jaundice. History of atopic dermatitis at 4 years of age which resolved on medication.
On examination, child was febrile and toxic. His vitals were stable. Generalised urticaria was present. Systemic examination showed soft tender hepatomegaly, liver span 11 cms.
His blood investigations showed - Haemoglobin: 12.6 g/dl; Haematocrit: 38.3 %; Platelet Count: 417.0 X 103/µl; RBC Count: 4.83 X 10×6/µl; Total WBC: 16.2 X 103/µl; ESR: 6 mm/hr; Peripheral smear: Normocytic normochromic RBCs with anisocytosis
Total Bilirubin (Serum): 4.83 mg/dl; Direct Bilirubin 4.33 mg/dl; Alanine Transaminase: 535.0 IU/L; Aspartate Transaminase: 286 IU/L; Alkaline Phosphatase :455 U/L; Total Protein (Serum): 6.80 G/dl; albumin (Serum): 3.30 g/dl; Globulin: 3.50 g/dl; Prothrombin Time: 13.4 Sec; INR: 1.20 LDH- 100IU/dL
Hepatitis-B Surface Antigen: Negative; Antibodies to Hepatitis C Virus: Non-Reactive; Anti IgM Hepatitis A Virus- Negative. Hepatitis E- negative. Antibodies to Leptospira (IgM): Negative; Standard agglutination test for Brucellosis: Negative; OX K: Negative; OX 19: Negative; OX 2: Negative; Scrub typhus IgM: Negative; Widal test: Negative; Anti-Dengue IgM: Negative Dengue Ns1Ag: Negative.
Blood culture was sterile. Serum Ceruloplasmin: 40 mg/dl. No KF ring,
G6PD- 28 IU/l (normal-8-18IU/L)
Covid-19 RTPCR- nasopharyngeal and oropharyngeal swab – Positive. SARS-CoV-2-Antibodies-negative
Ultrasound abdomen showed normal echotexture of liver. Autoimmune hepatitis panel (anti-nuclear antibody, anti-smooth muscle antibody, anti-liver kidney microsomal antibody) was negative.
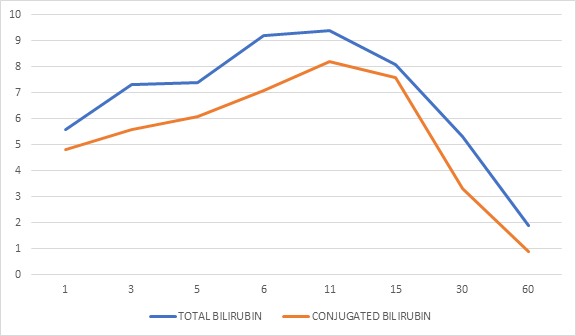
Patient was treated with intravenous fluids and multivitamins and choleretics. Hepatic Transaminases, ALT and AST showed peak increase around day 11 and gradual decline over 8 weeks (Figure 1) Serum ALP was only marginally elevated in comparison to the rise in Bilirubin and showed gradual decline over 8 weeks. Serum total bilirubin and conjugated bilirubin also decreased over a span of 8 weeks. (Figure 2)
Figure 1. Patient 1-Trend of Hepatic enzymes X axis- AST (BLUE) ALT( ORANGE) ALP( GREY)
Y axis- AST, ALT and ALP IU/L.
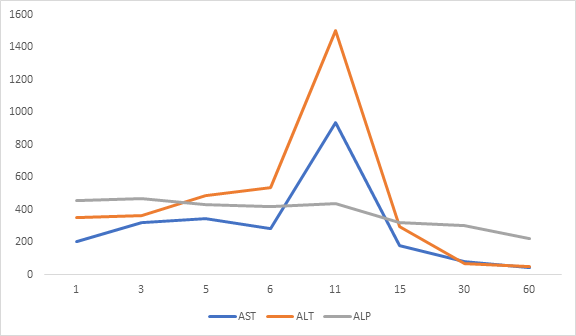
Figure 2. Patient 1-Trend of Serum Bilirubin Xaxis- Conjugated bilirubin( orange) total Bilirubin(blue)
Y axis- Bilirubin in mg/dl
Case 2
A 16-year-old female presented with fever for 8 days and rash for 3 days. At presentation she looked toxic with generalised urticaria. The rash started with face and progressed to involve the trunk, upper and lower limbs with sparing of genetalia and oral cavity. No history suggestive of upper or lower respiratory tract infection. No history of drug intake or travel. COVID vaccine was not given. On day 4 of admission, she developed jaundice with pruritis. Past history of atopic dermatitis 4 years back. No similar history of jaundice in the past. No family history of jaundice.
On examination she appeared toxic. She was hemodynamically stable. She had generalized urticaria scratch marks. Systemic examination showed soft, tender hepatomegaly, with liver span 13 cms.
Her blood investigations showed, Haemoglobin: 11 g/dl; Haematocrit:32.8 %; Platelet Count :1.54.0 X 10³/µl;RBC Count:3.98 X 10 × 6/µl; Total WBC: 5.9 X 103/µl; ESR: 32mm/hr; Peripheral smear: Normocytic normochromic RBCs with anisocytosis
Total Bilirubin (Serum): 5.22 mg/dl; Direct Bilirubin: 4.16 mg/dl; Alanine Transaminase: 298.0 IU/L; Aspartate Transaminase: 172 IU/L; Alkaline Phosphatase: 412 U/L; Total Protein (Serum): 1 g/dl; albumin (Serum): 3.50 g/dl; Globulin: 4.60 g/dl; Prothrombin Time: 12.4 Sec; INR: 1.10 LDH- 100 IU/dL
Hepatitis-B Surface Antigen: Negative; Antibodies to Hepatitis C Virus: Non-Reactive; Anti IgM Hepatitis A Virus- Negative. Hepatitis e- negative. Antibodies to Leptospira (IgM): Negative; Standard agglutination test for Brucellosis: Negative; OX K: Negative; OX 19:Negative; OX 2: Negative; Scrub typhus IgM: Negative; Widal test: Negative; Anti-Dengue IgM: Negative; Dengue Ns1Ag: Negative. Autoimmune hepatitis panel (anti-nuclear antibody, anti-smooth muscle antibody, anti-liver kidney microsomal antibody) was negative.
Serum Ceruloplasmin: 50mg/dl. No KF ring, G6PD- 42IU/l.
Ultrasound abdomen showed normal echotexture of liver. Blood culture was sterile.
COVID-19 RTPCR- nasopharyngeal and oropharyngeal swab - Positive.
SARS-CoV-2-Antibodies-negative
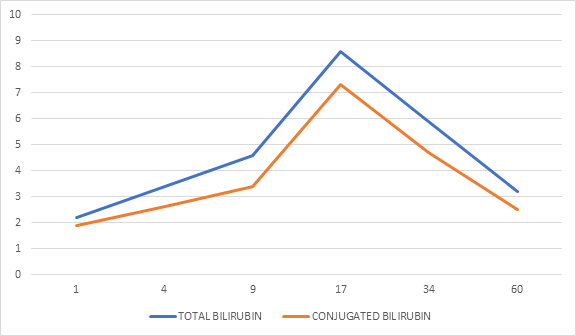
Patient was treated with intravenous fluids and multivitamins and Ursodeoxycholic acid. Transaminases, ALT, and AST showed peak increase around day 9, gradual decline over 8 weeks (Figure 3). Alkaline phosphatase showed gradual decline over 8 weeks. Serum total bilirubin and conjugated bilirubin, peaked around 2 weeks, with gradual decline over a span of 8 weeks (Figure 4).
Figure 3. Patient 2-Trend of Hepatic enzymes X axis- AST (BLUE) ALT(ORANGE) ALP (GREY)
Y axis - AST, ALT, and ALP IU/L.
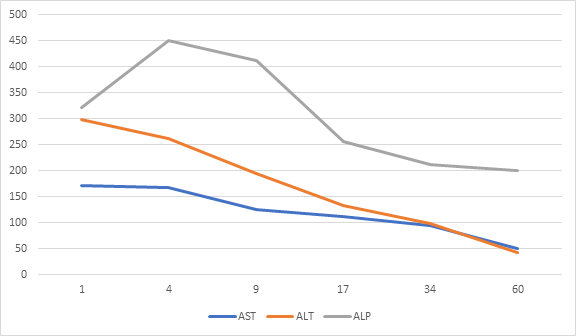
Figure 4. Patient 2 -Trend of Serum Bilirubin, Conjugated bilirubin( orange) total Bilirubin(blue)
Y axis- Bilirubin in mg/dl
| | | | Discussion | Liver involvement in the absence of pulmonary involvement in SARS-COV2 infection is very rarely reported in children. Hepatic involvement in the form of mild elevation of transaminases with normal synthetic function has been reported in Paediatric population.4 Severe hepatic disease with pulmonary involvement is seen in children with COVID -MISC or in severe SARS-COV2 infection with multiorgan involvement.1,3 Different mechanisms for liver injury in COVID-19 have been proposed including direct viral cytotoxic effect, mitochondrial protein interaction, endothelial dysfunction, and systemic inflammatory in response to the virus.5
COVID-19 virus causing cholestatic jaundice as the primary manifestation of SARS-COV2 infection is not yet reported in Paediatric population.
In both our patients COVID-19 RTPCR was positive, with serum negative for covid antibodies. They did not fulfill the criteria for COVID- MISC (fever for over 24 hours, elevated inflammatory markers, multisystem organ involvement, no alternative diagnoses, and past history of SARS-CoV-2 infection).6,7 The extensive blood investigations for all causes of primary liver disease were negative.
Hepatic involvement in both patients showed moderate elevation of transaminases with peak around 11th day and gradual decline over 8 weeks. Serum ALP, marker of cholestasis, was moderately raised in comparison with serum Bilirubin and declined in a similar pattern as transaminases. Serum bilirubin, both total and conjugated, showed similar gradual decline over 8 weeks. In other case series, severe elevation of hepatic enzymes has been reported and improvement was observed at 2 months. 8 Both the patients in the present case report, had normal coagulation profile with normal albumin indicating that synthetic liver function was not affected. In other case series8, synthetic liver function was affected with multiorgan involvement.
It is important to note that both the patients presented with fever and rash and had past history of atopic dermatitis. Other causes of endemic viral exanthems like Dengue, Scrub typhus were ruled out. None of the patients were on any medication. Whether past history of atopy predisposes to severe cholestatic hepatitis in COVID-19 is yet to be proved.
Both the patients were treated with supportive measures, choleretics, and fat-soluble vitamins. Both the patients were discharged after 3 weeks of admission.
What we know
• COVID-MISC or Severe SARS-CoV-2 infection with respiratory involvement can cause severe liver dysfunction
What is new?
• SARS-CoV-2 infection can cause severe cholestatic jaundice.
• Past history of atopic dermatitis can be a predisposing factor for cholestatic jaundice in COVID-19. However, further studies are required to prove this correlation.
• Complete resolution of liver biochemistry can take about 8 weeks in SARS-CoV-2 infection. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Perez A, Cantor A, Rudolph B, Miller J, Kogan-Liberman D, Gao Q, Da Silva B, Margolis KG, Ovchinsky N, Martinez M. Liver involvement in children with SARS-COV-2 infection: Two distinct clinical phenotypes caused by the same virus. Liver Int. 2021 Sep;41(9):2068-2075. doi: 10.1111/liv.14887. Epub 2021 Apr 22. PMID: 33826804; PMCID: PMC8251417. [CrossRef] [PubMed] [PMC free article]
- Saviano, A., Wrensch, F., Ghany, M.G. and Baumert, T.F. (2021), Liver Disease and Coronavirus Disease 2019: From Pathogenesis to Clinical Care. Hepatology, 74: 1088-1100. https://doi.org/10.1002/hep.31684. [CrossRef]
- Cantor A, Miller J, Zachariah P, DaSilva B, Margolis K, Martinez M. Acute Hepatitis Is a Prominent Presentation of the Multisystem Inflammatory Syndrome in Children: A Single-Center Report. Hepatology. 2020 Nov;72(5):1522-1527. doi: 10.1002/hep.31526. Epub 2020 Oct 27. PMID: 32810894; PMCID: PMC7655704. [CrossRef] [PubMed] [PMC free article]
- Bloom PP, Meyerowitz EA, Reinus Z, Daidone M, Gustafson J, Kim AY, Schaefer E, Chung RT. Liver Biochemistries in Hospitalized Patients With COVID-19. Hepatology. 2021 Mar;73(3):890-900. doi: 10.1002/hep.31326. Epub 2020 Nov 4. PMID: 32415860. [CrossRef] [PubMed]
- Sultan S, Altayar O, Siddique SM, Davitkov P, Feuerstein JD, Lim JK, Falck-Ytter Y, El-Serag HB; AGA Institute. Electronic address: ewilson@gastro.org. AGA Institute Rapid Review of the Gastrointestinal and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology. 2020 Jul;159(1):320-334.e27. doi: 10.1053/j.gastro.2020.05.001. Epub 2020 May 11. PMID: 32407808; PMCID: PMC7212965. [CrossRef] [PubMed] [PMC free article]
- Feldstein LR, Tenforde MW, Friedman KG, et al. Characteristics and Outcomes of US Children and Adolescents With Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA. 2021;325(11):1074-1087. doi:10.1001/jama.2021.2091. [CrossRef]
- Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, Ladisch S, McClain K, Webb D, Winiarski J, Janka G. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007 Feb;48(2):124-31. doi: 10.1002/pbc.21039. PMID: 16937360. [CrossRef] [PubMed]
- Antala S, Diamond T, Kociolek LK, Shah AA, Chapin CA. Severe Hepatitis in Pediatric Coronavirus Disease 2019. J Pediatr Gastroenterol Nutr. 2022 May 1;74(5):631-635. doi: 10.1097/MPG.0000000000003404. PMID: 35149651; PMCID: PMC9117453. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2026.66
|
| Cite this article as: | | Moras K J, Mundkur S C, Periera R A. Cholestatic Jaundice in Pediatric COVID-19: two case reports. Pediatr Oncall J. 2024 May 03. doi: 10.7199/ped.oncall.2026.66 |
|