Teresa Cachada Baptista, Manuel Lima Ferreira, Bárbara Costa Correia, Susana Lira, Leonilde Machado.
Paediatrics and Neonatology Department, Unidade Local de Saúde de Tâmega e Sousa, 4564-007 Penafiel, Portugal.
ADDRESS FOR CORRESPONDENCE
Ana Teresa Sá Cachada Baptista, Travessa de Vilar nº 77, 4595-085, Eiriz, Paços de Ferreira, Porto, Portugal.
Email: atscbaptista@gmail.com | | Keywords | | Ataxia, Neuroblastoma, Opsoclonus-myoclonus syndrome, Saccadic eye movements. | | | Opsoclonus-myoclonus syndrome (OMS) is a rare immune-mediated neurological disorder marked by chaotic eye movements, myoclonus, trunk instability, behavioral changes, and sleep disturbances.1,2 Often linked to neuroblastoma, OMS can also follow infections like respiratory syncytial virus, rhinovirus, SARS-CoV-2, or Epstein-Barr virus.1,2,3 Diagnosis is clinical.1,2,4
A previously healthy 10-month-old male infant with normal psychomotor development presented to a level II Emergency Department (ED) with a 2-day history of fever (peak 39.6 °C), intermittent irritability, and neurodevelopmental regression, notably loss of independent sitting, accompanied by head tremor and eyelid fluttering. Over the preceding 10 days, he exhibited partial feeding refusal and had been assessed in ED on Days (D) 1 and D5, with unremarkable physical and laboratory findings. On D10, clinical evaluation revealed a fair general state, persistent irritability with episodes of inconsolable crying, inability to sit unaided, truncal and head titubation, axial ataxia, and chaotic, multidirectional saccadic eye movements. Laboratory tests were within normal limits (Table 1).
Table 1. Results of blood tests carried out in the emergency department.
| Blood Test |
Result |
Normal Range |
| Hemoglobin |
11.6 g/dL |
11.3-13.3 g/dL |
| Leukocytes |
10980/uL |
6000-160000/uL |
| Neutrophils |
3950/uL |
1000-8000/uL |
| Lymphocytes |
5150/uL |
3400-10050/uL |
| Platelets |
238000/uL |
200000-500000/uL |
| Glucose |
85 mg/dL |
76-110 mg/dL |
| Urea |
16 mg/dL |
10-34 mg/dL |
| Creatinine |
0.41 mg/dL |
0.4-0.7 mg/dL |
| Sodium |
135 mmol/L |
136-146 mmol/L |
| Potassium |
4.7 mmol/L |
4.1-5.3 mmol/L |
| Chlorine |
107 mmol/L |
101-109 mmol/L |
| Aspartate Aminotransferase |
54 UI/L |
<82 UI/L |
| Alanine Aminotransferase |
26 UI/L |
<54 UI/L |
| Creatine phosphokinase |
157 UI/L |
50-300 UI/L |
| C-Reactive Protein |
<5 mg/L |
<5 mg/L |
| Procalcitonin |
<0.5 ng/mL |
<0.5 ng/mL |
| Alpha-fetoprotein |
9,8 ng/mL |
<9 ng/mL |
| Neuronal-specific Enolase |
184.6 ng/mL |
0-15.2 ng/mL |
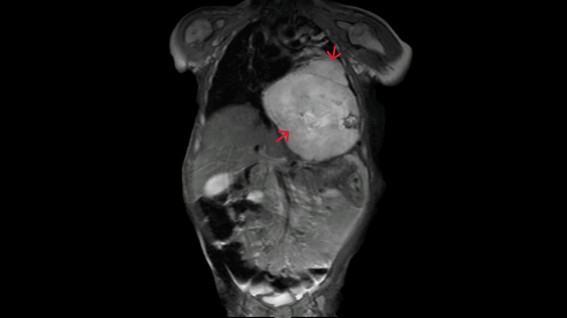
Serologies were negative, blood cultures pending, and neuron-specific enolase elevated (184.6 ng/mL). Cranial computed tomography (CT) was normal. Lumbar puncture revealed normal cytochemical analysis; cerebrospinal fluid (CSF) viral studies were negative, and bacterial culture of CSF was pending. Intravenous ceftriaxone and acyclovir were started. Due to clinical suspicion of OMS, the patient was admitted for further evaluation. MRI revealed a large mass occupying the lower two-thirds of the left hemithorax, without peripheral invasion, suggestive of neuroblastoma or teratoma (Figure 1). He was subsequently transferred to a tertiary center, where imaging favored neuroblastoma.
Figure 1. Thoraco-abdominal-pelvic magnetic resonance imaging showing neuroblastoma in the coronal plane.
Urinary catecholamines were elevated on D13. Fine-needle aspiration biopsy on D14 confirmed neuroblastoma histology. By D15, both blood and CSF cultures remained to have no growth. Absence of MYCN amplification was confirmed by D20. MIBG scintigraphy demonstrated intense uptake localized to the tumor, with no evidence of metastasis. Antibiotic and antiviral therapies were discontinued, and systemic corticosteroids initiated, followed by chemotherapy. This regimen resulted in marked neurological improvement.
This case highlights opsoclonus-myoclonus syndrome (OMS), a rare pediatric neuroinflammatory disorder with an incidence of 0.27-0.40 per million annually, primarily affecting children around 18 months.1,2 OMS presents with subacute ataxia, truncal instability, titubation, and often myoclonus, tremor, or hypotonia.1 Early diagnosis is challenging as hallmark opsoclonus may be initially absent.1 Behavioral disturbances and developmental regression are common, sometimes preceded by nonspecific prodromal symptoms.1,2 Due to its strong paraneoplastic link, especially with neuroblastoma, thorough oncologic assessment—including MRI of thorax, abdomen, pelvis, urinary catecholamines (VMA/HVA), and MIBG scintigraphy-is crucial despite false negatives in low-grade tumors lacking MYCN amplification.1,2,5
Diagnosis is clinical, supported by cerebrospinal fluid analysis, virologic/bacteriologic studies, and brain MRI to exclude other etiologies as post-infectious cause, post-vaccination response, autoimmune ataxias and viral or autoimmune encephalitis.1,2 Prompt immunosuppression with corticosteroids and ivig is essential, with rituximab or cyclophosphamide added if refractory. Treatment targets remission and sustained immunosuppression for up to a year.1,2 Neurologic recovery varies: motor symptoms improve in 60%, yet cognitive and behavioral deficits persist in up to 80%. Early recognition is key for optimal outcomes.1,2 | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Rossor, T., Yeh, E. A., Khakoo, Y., Angelini, P., Hemingway, C., Irani, S. R., Schleiermacher, G., Santosh, P., Lotze, T., Dale, R. C., Deiva, K., Hero, B., Klein, A., de Alarcon, P., Gorman, M. P., Mitchell, W. G., Lim, M., & OMS Study Group (2022). Diagnosis and Management of Opsoclonus-Myoclonus-Ataxia Syndrome in Children: An International Perspective. Neurology(R) neuroimmunology & neuroinflammation, 9(3), e1153. https://doi.org/10.1212/NXI.0000000000001153. [CrossRef] [PubMed] [PMC free article]
- Hsu, M., Tejani, I., Shah, N., Olaosebikan, R., Kumar, A., & Naik, S. (2024). Review of Opsoclonus-Myoclonus Ataxia Syndrome in Pediatric Patients. Children, 11(3), 367. https://doi.org/10.3390/children11030367. [CrossRef] [PubMed] [PMC free article]
- Rothenberg, A. B., Berdon, W. E., D'Angio, G. J., Yamashiro, D. J., & Cowles, R. A. (2009). The association between neuroblastoma and opsoclonus-myoclonus syndrome: a historical review. Pediatric radiology, 39(7), 723-726. https://doi.org/10.1007/s00247-009-1282-x. [CrossRef] [PubMed]
- Matthay, K. K., Blaes, F., Hero, B., Plantaz, D., De Alarcon, P., Mitchell, W. G., Pike, M., & Pistoia, V. (2005). Opsoclonus myoclonus syndrome in neuroblastoma a report from a workshop on the dancing eyes syndrome at the advances in neuroblastoma meeting in Genoa, Italy, 2004. Cancer letters, 228(1-2), 275-282. https://doi.org/10.1016/j.canlet.2005.01.051. [CrossRef] [PubMed]
- Brunklaus, A., Pohl, K., Zuberi, S. M., & de Sousa, C. (2012). Investigating neuroblastoma in childhood opsoclonus-myoclonus syndrome. Archives of disease in childhood, 97(5), 461-463. https://doi.org/10.1136/adc.2010.204792. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2026.80
|
| Cite this article as: | | Baptista T C, Ferreira M L, Correia B C, Lira S, Machado L. Opsoclonus-Myoclonus-Syndrome – A Cause Never To Be Forgotten. Pediatr Oncall J. 2025 Dec 15. doi: 10.7199/ped.oncall.2026.80 |
|