Catarina Martins, Inês Mazeda, Sofia Gonçalves Macedo, Inês Vivas, Maria José Dinis.
Pediatrics and Neonatology Department, Unidade Local de Saúde de Póvoa de Varzim/Vila do Conde, Portugal.
ADDRESS FOR CORRESPONDENCE
Catarina Martins, Largo da Misericórdia, 4490-421, Póvoa de Varzim, Portugal.
Email: catarinaguimm@gmail.com | | Keywords | | Lipschutz ulcer, Infections, Hyperpigmented lesions, Adolescents, Non-sexually transmitted | | | | Introduction | | Lipschütz ulcer is a rare, non-sexually transmitted condition that typically affects healthy young females.1 Although the etiology remains unclear, it is frequently associated with viral infections such as Epstein-Barr virus or bacterial agents like Campylobacter jejuni.2 Clinically, it presents as a painful, necrotic and rapidly appearing ulcer in the vulvar or lower vaginal region and may be accompanied by systemic symptoms including fever, myalgia, or sore throat.2,3 The diagnosis is clinical and requires exclusion of other causes of genital ulcers, such as herpes simplex, syphilis, autoimmune diseases, or adverse drug reactions.4 Management is supportive, focusing on symptom relief with analgesics and local care.4 In most cases, the ulcers resolve spontaneously within 2–3 weeks without recurrence or long-term sequelae, but in cases of intense pain, systemic corticosteroids can be administered.3,5 | | | | Case Report | Case 1
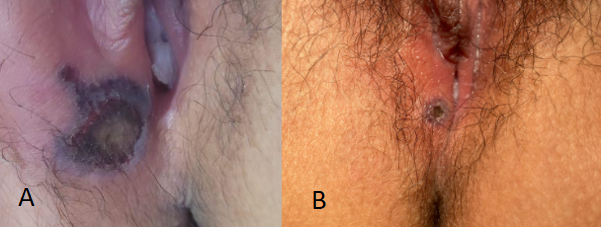
An 11-year-old adolescent was observed in the emergency department for a lesion in the vulvar region, without associated pain or pruritus. On physical examination, a small vulvar ulcer with hyperpigmentation was noted at the level of the fourchette, lateralized to the right (Figure 1 - Panel A). A sample of the ulcer exudate was collected, along with serological tests: screening for sexually transmitted diseases was negative, CMV was negative, EBV VCA IgG >320.00 U/mL, and EBV EBNA IgG >320.00 U/mL. Immunoglobulin levels and an autoimmune study were also requested, revealing only a C4 level of 50.1 mg/dL and IgE of 381 IU/mL. A diagnosis of Lipschütz ulcer was made, and the patient was discharged with local analgesics, flucloxacillin, and corticosteroid therapy, with progressive reduction of the lesion (Figure 1 - Panel B).
Figure 1. Panel A - Small vulvar ulcer with hyperpigmentation at the level of the fourchette, lateralized to the right; Panel B - vulvar ulcer with hyperpigmentation with progressive reduction.
Case 2
A 15-year-old adolescent was evaluated in the emergency department for odynophagia, anterior rhinorrhea, and hoarseness with approximately three days of evolution. Additionally, she had a fever for about two days, with afebrile intervals every four hours and a recorded maximum temperature of 39ºC. On the same day, she also reported the appearance of hard, painless vulvar lesions, without other gynecological complaints
On physical examination, two ulcerated and darkened vulvar lesions were noted on the right side, measuring approximately 2 cm and 1 cm, respectively, and painless to touch (Figure 2). Serological tests for HIV, EBV, CMV, and VDRL were performed, all yielding negative results.
She was discharged with topical lidocaine and hydrocortisone treatment and was reevaluated about two weeks later, showing significant clinical improvement and regression of the lesions.
Figure 2. Two ulcerated and darkened vulvar lesions.
 | | | | Discussion | The two cases presented illustrate the clinical heterogeneity of this condition, emphasizing differences in symptomatology, serological findings, and treatment response.
The first case describes an 11-year-old girl with a solitary, painless ulcer discovered incidentally during examination, whereas the second case involved a 15-year-old adolescent with systemic symptoms, including fever, odynophagia, and rhinorrhea, followed by the sudden onset of vulvar ulcers. These contrasting presentations highlight the spectrum of clinical manifestations of Lipschütz ulcers, ranging from asymptomatic localized lesions to cases associated with systemic viral-like symptoms.1,2,6
Pain and pruritus are common but not universal features of this condition. Case 1 lacked pain or systemic symptoms, while case 2 presented with fever and pharyngitis, supporting previous reports of a possible viral prodrome preceding ulcer formation.3,6
Lipschütz ulcers have been linked to viral infections, particularly Epstein-Barr virus (EBV), cytomegalovirus (CMV), and other immune-mediated responses.3,7 The first patient exhibited a strong EBV serological response (high EBV VCA IgG and EBNA IgG levels), suggesting a post-viral immune reaction, while the second patient tested negative for EBV, CMV, and other infectious causes. This discrepancy suggests that while EBV is a common associated factor, it is not the sole cause, and other infectious or immune-mediated pathways may contribute to ulcer development.3,6,8
Interestingly, the first case also showed elevated IgE and decreased C4 levels, which could suggest a role for immune dysregulation in ulcer formation. The significance of these findings remains unclear, but they align with previous reports of transient immune alterations in patients with Lipschütz ulcers.2,6,4
Both cases underwent extensive infectious disease screening, including HIV, syphilis (VDRL), CMV, and EBV, reinforcing the diagnosis of exclusion characteristic of Lipschütz ulcers. Given that these ulcers can mimic sexually transmitted infections (STIs), thorough serological testing is crucial to avoid misdiagnosis and unnecessary concern regarding sexual abuse, particularly in pediatric patients.1,6
Beyond infectious causes, autoimmune conditions such as Behçet’s disease and reactive arthritis should also be considered in recurrent or atypical cases.3 However, the self-limited nature of the ulcers in both patients, with full resolution within weeks, strongly supports Lipschütz ulcer as the most plausible diagnosis. The differential diagnosis of acute genital ulcers in non-sexually active girls remains challenging and often leads to delayed recognition of this benign, self-limited entity.7,8
Both patients responded well to symptomatic treatment with topical analgesics (lidocaine), corticosteroids, and, in one case, flucloxacillin. The addition of antibiotics in case 1 was likely a precautionary measure rather than a necessity, asbacterial superinfection is rare. Given that Lipschütz ulcers are self-limiting, a conservative approach is often sufficient, reserving systemic therapy (e.g., corticosteroids) for severe or extensive cases.3,5 | | | | Conclusion | | Lipschütz ulcer is a rare, self-limited condition that may be underrecognized due to its overlap with other causes of genital ulceration, including sexually transmitted infections. While its pathogenesis is not fully understood, a strong association with viral or bacterial infections has been established. The diagnosis is clinical and supported by exclusion of other etiologies. The two cases described highlight the diversity of clinical presentations and reinforce the importance of awareness among healthcare providers to avoid unnecessary treatments and invasive investigations. Further studies are needed to better understand the disease’s pathophysiology and identify potential diagnostic biomarkers. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Govindan B. Lipschütz ulcers: a literature review based on 79 cases. EMJ Reprod Health. 2016;2(1):73-8. [CrossRef]
- Vismara SA, Lava SAG, Kottanattu L, et al. Lipschütz's acute vulvar ulcer: a systematic review. Eur J Pediatr. 2020;179(10):1559-67. doi:10.1007/s00431-020-03647-y. PMID:32296983. [CrossRef] [PubMed]
- Sadoghi B, Stary G, Wolf P, et al. Ulcus vulvae acutum (Lipschütz): a systematic literature review and a diagnostic and therapeutic algorithm. J Eur Acad Dermatol Venereol. 2020;34(7):1432-9. doi:10.1111/jdv.16161. [CrossRef] [PubMed] [PMC free article]
- Huppert JS. Lipschütz ulcers: evaluation and management of acute genital ulcers in women. Dermatol Ther. 2010;23(5):533-40. doi:10.1111/j.1529-8019.2010.01356.x. [CrossRef] [PubMed]
- González L, Cuéllar L, Ríos M, et al. Úlcera de Lipschütz: una causa poco conocida de úlceras vulvares. An Pediatr (Barc). 2010;73(5):269-71. doi:10.1016/j.anpedi.2010.06.008. [CrossRef] [PubMed]
- Rosman IS, Berk DR, Bayliss SJ. Acute genital ulcers in nonsexually active young girls: case series, review of the literature, and evaluation and treatment recommendations. Pediatr Dermatol. 2012;29(2):147-53. doi:10.1111/j.1525-1470.2011.01515.x. [CrossRef] [PubMed]
- Vieira-Baptista P, Lima-Silva J, Beires J, et al. Acute vulvar ulcers: why is this diagnosis still a challenge? Eur J Obstet Gynecol Reprod Biol. 2018;220:115-20. doi:10.1016/j.ejogrb.2017.11.014. [CrossRef] [PubMed]
- Le Cleach L, Truchetet F, et al. Painful acute genital ulcers in women: diagnosis and treatment. Dermatol Clin. 2021;39(3):431-42. doi:10.1016/j.det.2021.02.010.
DOI: https://doi.org/10.7199/ped.oncall.2026.88
|
| Cite this article as: | | Martins C, Mazeda I, Macedo S G, Vivas I, Dinis M J. Lipschütz Ulcers in adolescents: report of two pediatric cases. Pediatr Oncall J. 2026 Jan 17. doi: 10.7199/ped.oncall.2026.88 |
|