Sriparna Basu1, Amrita Ghosh Kar2, Arti Mata3, S. Gupta1, Ashok Kumar1, B.D. Bhatia1.
1Departments of Pediatrics, Institute of Medical Sciences, Banaras, India,
2Departments of Pathology, Institute of Medical Sciences, Banaras, India,
3Departments of Gynae and Obstetrics, Institute of Medical Sciences, Banaras, India.
ADDRESS FOR CORRESPONDENCE
Dr. Sriparna Basu, Department of Pediatrics, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005. India.
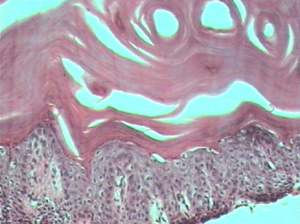
Email: drsriparnabasu@rediffmail.com | | Abstract | | Harlequin ichthyosis is the most severe form of congenital ichthyosis. It is a rare autosomal recessive disorder (1:300,000) and common in consanguineous marriages (1). The skin development is altered in utero due to defective lipid metabolism in lamellar granules of the keratinocytes. The primary defect lies in the protein phosphatase activity. Lack of desquamation and massive accumulation of scales leads to the characteristic morphological features. We report a case of harlequin ichthyosis who had a history of similar affection in two earlier siblings. | | | | Keywords | | Harlequin fetus, ichthyosis | | | | Case Report | A full term male baby, product of a non-consanguineous marriage was born to a 30-year-old multigravida (G4, P3+1) by breech extraction. The antenatal period was uneventful and the baby cried immediately after birth. His anthropometric measurements were birth weight - 2.32 kg, crown heel length - 43 cm, head / chest circumference - 32/29 cm. On examination the skin of the baby was leathery white with large shiny plaques separated by deep erythematous fissures along with flexion contractures of arms, legs and digits. He also had severe ectropion, rudimentary pinna, sparse hairline at the back of the scalp, nasal hypoplasia and eclabium with a fixed, open mouth (Fig.1). Fingers and toes were hypoplastic and tips were gangrenous. All natural orifices were patent. External genitalia were male with bilateral undescended testes. Umbilical cord was fragile. The vital parameters were within normal limits except mild tachypnea (68/min). Infantogram was normal. Ultrasonography of abdomen and neurosonogram did not reveal any abnormality. Skin biopsy showed massive hyperkeratosis associated with normal granular cell layer and dilated spaces in the stratum corneum representing the ostia of eccrine sweat ducts [Fig. 2]. With these findings a diagnosis of harlequin ichthyosis was made. On interrogation, mother gave past history of similar affection in the first and the third issues who died at home within few hours after birth while the second is a normal living male child of 7 years. The baby was managed in nursery with symptomatic and supportive measures. Parents refused for Karyotyping and absconded with the baby on 5th day of life.
Fig 1. Harlequin fetus

Fig 2. Skin biopsy: Massive hyperkeratosis associated with normal granular cell layer. The dilated spaces in the stratum corneum represent the ostia of eccrine sweat ducts. (H&E, 40x)
 | | | | Discussion | Harlequin babies are born with dense plaque-like scales forming a massive horny shell around their body. These scales or plaques measure up to 4-5 cm on a side and are usually diamond or triangular shaped. 'Splits' between these scales reveal erythematous moist fissures, whose bright red color is in sharp contrast to the lighter colored scales. This shell impedes movement, and the fissures cause the protective skin barrier to be compromised, thus leaving the fetus susceptible to dehydration and infection. Because of the scaling of the skin, the limbs are often deformed to the extent that movement is restricted, and may be undersized and incompletely formed. The scales may sometimes also constrict blood flow to the limbs resulting in swelling or in severe cases, gangrene (2).
Abnormalities of skin is linked to the abnormal structure and function of lamellar granules originating from the Golgi apparatus of keratin-producing cells in the horny outer layer of the epidermis, whose function is to secrete lipids that maintain the skin barrier. Harlequin fetuses either do not have these granules, or have defective ones, which results in massive loss of water between the layers of skin. The lack of a class of enzymes known as hydrolases further prevents shedding of skin cells, thus causing overgrowth of the horny layer of skin (3). The genetic and biochemical basis is poorly understood. A mutation of ABCA 12 gene on chromosome 2 has been reported (4). Ultrasonography can make a prenatal diagnosis and should be used particularly in those families with history of a Harlequin baby (5).
Our patient had the typical phenotypic features of a Harlequin fetus. The skin biopsy was also diagnostic. Though USG in expert hands during the antenatal period is diagnostic of the condition the family did not go for any antenatal check up because of social taboos. Even in the present pregnancy they were quite reluctant to reveal previous affections. History of consanguinity was absent in our patient. Karyotyping and mutational analysis could have revealed some abnormality but these were again refused.
Treatment of harlequin babies can be done with a battery of medications ranging from oral retinoids to antiseptics and topical paraffin ointments to soften the skin. In general, harlequin fetuses do not survive for long. Death is often due to dehydration, systemic infection or impaired respiration.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Sarkar R, Sharma RC, Sethi S, et al. Three unusual siblings with Harlequin ichthyosis in an Indian family. J Dermatol 2000; 27:609-11. [CrossRef] [PubMed]
- Murphy-Brown L, Vella JA, Lawlor-Klean P. Harlequin ichthyosis: a case study. Neonatal Netw 2004; 23:7-12. [CrossRef] [PubMed]
- Akiyama, M. The pathogenesis of severe congenital ichthyosis of the neonate. J Dermatol Sci 1999; 21: 96-104. [CrossRef]
- Layton J. A review of Harlequin ichthyosis. Neonatal Netw 2005; 24:17-23. [CrossRef] [PubMed]
- Berg C, Geipl A, Kohl M, et al. Prenatal sonographic features of Harlequin ichthyosis. Arch Gynecol Obstet 2003; 268:48-51. [PubMed]
|
| Cite this article as: | | Basu S, Kar A G, Mata A, Gupta S, Kumar A, Bhatia B. Harlequin Ichthyosis. Pediatr Oncall J. 2007;4: 53. |
|