Amit Agrawal, Akshay Pratap, Nisha Bhatta, Anand Kumar.
Department of Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
ADDRESS FOR CORRESPONDENCE
Dr. Amit Agrawal, Assistant Professor in Neurosurgery, Department of Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
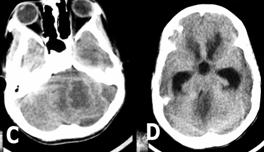
Email: dramitagrawal@gmail.com | | Abstract | | The infratentorial variety of the subdural empyema, with coexisting cerebellar abscess, is a rare clinical entity that carries a high mortality rate. Clinical presentation of infratentorial subdural empyema encompasses a systemic febrile illness, headaches, and a stiff neck. The diagnosis is frequently delayed and often confused with that of meningitis. Cerebrospinal fluid analysis will confirm the diagnosis of meningitis in majority of the cases and will further delay the diagnosis as in present case. | | | | Keywords | | Subdural empyema, mastoiditis, cerebellar abscess | | | | Introduction | | Since the introduction of antibiotic therapy, the percentage of intracranial complications from otitic disease has decreased, although they still represent a challenge for early recognition, adequate treatment, and satisfactory results (1-3). Infratentorial empyema is an uncommon form of intracranial suppuration that is usually secondary to neglected otogenic infection (4,5). The infratentorial variety of the subdural empyema, with coexisting cerebellar abscess, is a rare clinical entity that carries a high mortality rate (6). We report such a case. | | | | Case Report | This 13 years child presented with fever and headache of 21 days duration, neck stiffness of 18 days duration and limbs stiffness of 18 days duration. Fever was continuous, moderately high grade with chills and rigors. The patient was treated at local hospital and a diagnosis of meningitis was made. CT scan plain and contrast done at that time showed thin subdural collection over left cerebellar hemisphere (Figure-1). With that lumbar puncture was performed and it showed 480 cells (polymorphs-70%, lymphocyte-30%). Protein was 280 mg% and sugar was 10 mg% which further confirmed the diagnosis of meningitis. He was on broad spectrum antibiotics but did not improve. After three days, he suddenly deteriorated in sensorium and became drowsier. He developed increased stiffness of all four limbs. An immediate repeat CT scan was performed and it showed increase in the size of subdural empyema and a thin-walled large cerebellar abscess with severe oedema and massive hydrocephalus (Figure-2). He had history of chronic otitis media since childhood and he was dumb since birth. On examination he had excessive salivation and weak cough. On chest examination he had bilateral crepitations. Neurologically he was in altered sensorium and moving all four limbs. Before suboccipital craniectomy, he underwent right frontal external ventricular drainage. CSF was clear and under high pressure. Following that he underwent left paramedian suboccipital craniectomy and evacuation of subdural empyema and cerebellar abscess. Culture showed Acinetobacter species (resistant to all antibiotics) and Pseudomonas (sensitive to chloramphenicol). He was continued with broad spectrum antibiotics (Ceftriaxone, amikacin, metronidazole). He continued to deteriorate in his neurological status and developed aspiration pneumonitis and succumbed to it.
Figure-1. Contrast CT showing subdural empyema over left cerebellar hemisphere with mid ipsilateral cerebellar oedema
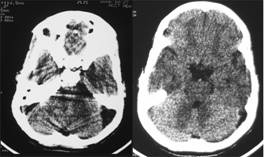
Figure-2. Repeat CT showing massive increase in the size of empyema with left cerebellar abscess, diffuse cerebellar oedema and obstructive hydrocephalus
 | | | | Discussion | | Main causes of posterior fossa subdural empyema are otitis media and mastoiditis (7-9). Several veins and venules in the middle ear normally communicate through intact bone and dura with vessels in the subarachnoid space and brain parenchyma. Micro organisms can spread through these veins and reach the subdural and subarachnoid spaces by mechanisms of thrombophlebitis and periphlebitis (10, 11). Clinical presentation of infratentorial subdural empyema encompasses a systemic febrile illness, headaches, and a stiff neck. The diagnosis is frequently delayed and often confused with that of meningitis (4, 5). Cerebrospinal fluid analysis will confirm the diagnosis of meningitis in majority of the cases and will further delay the diagnosis as in present case. Computerized tomography will allow a precise diagnosis and localization of the pathology (4). On CT scan, these lesions usually appears as a thin rim of fluid slightly hyperdense to cerebrospinal fluid (CSF) with surrounding enhancement, adjacent disproportionate cortical edema and effacement of cortical sulci (4, 12, 13). Investigations including computerized tomography (CT) scans may sometime equivocal and diagnosis can be delayed (9). Early aggressive surgical interventions in such cases should result in a minimal morbidity. Urgent evacuation of infected material by a neurosurgeon and otolaryngologist team either simultaneously or at the earliest possible opportunity for eradicating the source of infection results in cure and a significant decrease in recollection and re-exploration (13-15). Early surgical drainage via wide posterior fossa craniectomy, aggressive treatment of associated hydrocephalus, eradication of the primary source of sepsis, and, finally, intravenous high dosage of appropriate antibiotics (for 6 weeks) form the mainstay of treatment (4-6, 9). Delay in surgery will lead to clinical worsening and poor results (4, 5). Patients operated within 72 hours had 10% disability as against 70% if the surgery took place after 72 hours (16). Although rare, infratentorial empyema, especially when subdural, is a lethal disease (5). The severity of these complications as in present case underlines the importance of clinical awareness, high index of suspicion and early imaging diagnosis to establish suitable treatment. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Penido Nde O, Borin A, Iha LC, Suguri VM, Onishi E, Fukuda Y, Cruz OL. Intracranial complications of otitis media: 15 years of experience in 33 patients. Otolaryngol Head Neck Surg. 2005; 132(1):37-42. [CrossRef] [PubMed]
- Kolenda J, Carr MM, Lemckert RJ, Ummat SK. Intracranial sinus thrombosis secondary to ear disease in an adolescent. J Otolaryngol 1997; 26:203-206. [PubMed]
- Kuczkowski J, Mikaszewski B. Intracranial complications of acute and chronic mastoiditis: report of two cases in children. Int J Pediatr Otorhinolaryngol 2001; 60:227-237. [CrossRef]
- Borovich B, Johnston E, Spagnuolo E. Infratentorial subdural empyema: clinical and computerized tomography findings. Report of three cases. J Neurosurg. 1990; 72(2):299-301. [CrossRef] [PubMed]
- Nathoo N, Nadvi SS, van Dellen JR. Infratentorial empyema: analysis of 22 cases. Neurosurgery. 1997; 41(6):1263-8. [CrossRef] [PubMed]
- Polyzoidis KS, Vranos G, Exarchakos G, Argyropoulou MI, Korantzopoulos P, Skevas A. Subdural empyema and cerebellar abscess due to chronic otitis media. Int J Clin Pract. 2004; 58(2):214-7. [CrossRef] [PubMed]
|
| Cite this article as: | | Agrawal A, Pratap A, Bhatta N, Kumar A. Subdural Empyema and Cerebellar Abscess in a Child due to Chronic Otitis Media. Pediatr Oncall J. 2007;4. |
|