Department Of Paediatrics, Kasturba Medical College, Manipal, India.
ADDRESS FOR CORRESPONDENCEDr Dinesh Nayak, Associate Professor, Department Of Paediatrics, Kasturba Medical college, Manipal -576104. India.
Email: A 15-year-old girl was admitted to our hospital with a history of sudden onset of severe headache in the occipital and bifrontal areas with associated symptoms of nausea and vomiting and also low grade fever, two weeks prior to hospitalization. No history of previous trauma was reported. On examination, her BP was normal, no neurocutaneous markers. Findings of the neurologic examinations performed during the patient's hospital admissions were within normal limits except for retrocollis. Rest of the systemic examination was essentially normal. Cervical spine X-ray revealed hyperextension without any bony abnormalities. Her chest X-ray was unremarkable. Mantoux test revealed no induration at the end of 48 hours. Ensuring that there was no papilloedema or no significant cerebral edema, a cerebrospinal fluid analysis was performed, which revealed xanthochromia suggestive of subarachnoid haemorrhage. Contrast enhance CT of the brain obtained on hospital admission showed a rounded well defined extra-axial lesion anterolateral to pons arising from the basilar artery (BA) and was reported as partially thrombosed aneurysm. MRI which was performed subsequently better delineated the aneurysm.(Fig 1a and 1b) Digital subtraction angiography of the brain performed 6 days later confirmed a large saccular aneurysm with irregular outline arising from the posterior wall of the mid portion of the BA .(Fig 2) The aneurysm was seen to arise proximal to the origin of both superior cerebellar arteries and the mid portion of the BA showed narrowing likely due to spasm. Other investigations such as lipid profile, prothrombin time, activated partial thromboplastin time, complete blood counts and erythrocyte sedimentation rate were normal. A right fronto-temporal craniotomy with microsurgical endoluminal muscle packaging of giant BA aneurysm sac was done. A CT scan obtained immediately after the operation demonstrated residual aneurysm filled with muscle packing. Post operative patient recovery was uneventful except that she developed left hemiparesis. The patient was discharged 15 days after surgery with significant improvement and was able to walk with support. The patient was advised to continue physiotherapy and advised to come for follow up 6 weeks later for cerebral angiography.
Figure 1a and 1b: Axial and Sagittal T1 weighted MR images show partially thrombosed aneurysm causing significant compression of the pons anteriorly (arrows).

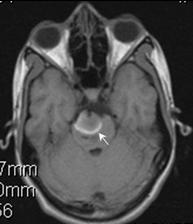 Fig 2: Digital subtraction angiography of the posterior circulation acquired in lateral projection shows saccular aneurysm (arrowhead) arising from the mid basilar artery (arrow) directed superiorly and laterally.
Fig 2: Digital subtraction angiography of the posterior circulation acquired in lateral projection shows saccular aneurysm (arrowhead) arising from the mid basilar artery (arrow) directed superiorly and laterally.

Most true aneurysms are congenital in nature, although their appearance in childhood is uncommon. (1) Aneurysms increase in frequency with age beyond the third decade, are 1.6 times more common in women and are associated with a number of genetic conditions. Prospective autopsy and angiographic studies indicate that between 3.6 and 6% of the population harbor an intracranial aneurysm .(2) Cerebral aneurysms usually occur in the Circle of Willis at the bifurcation of arteries, with approximately 33% arising at the anterior communicating artery, 33% at the origin of posterior communicating artery, 20% at the middle cerebral artery and only 14% involving the vertebral and basilar circulation .(1) Intracranial aneurysms are seldom encountered in the pediatric age group, and those within the posterior circulation are even rarer .(2-4) Pediatric intracranial aneurysms occur more commonly in male patients and have a predilection for the terminal internal carotid artery bifurcation.(5)
Giant aneurysms carry a severe morbidity and mortality rate because of the tendency to cause distal thromboembolism (6). The subarachnoid hemorrhage (SAH) occurring mostly due to rupture of an intracranial aneurysm accounts for a quarter of cerebrovascular deaths. (7) Although the most common presentation of a cerebral aneurysm is with subarachnoid haemorrhage, unruptured cerebral aneurysms may present with headache or other symptoms, in particular neuro-ophthalmological features .(8) Clinical presentation is usually related to mass effect associated with large aneurysms or intracranial hemorrhage. Spontaneous thrombosis of intracranial aneurysms is uncommon, very rare in children but also has been occasionally described .(3,9-11) It has been proposed that thrombosis is not the usual final stage of the aneurysm evolution, but rather an ongoing dynamic process that has potential for further growth and mass effect. Aneurysmal growth may be due to accumulation of thrombotic materials, recurrent intramural hemorrhage, or development of intrathrombotic capillary channels, which may, in turn, thrombose or bleed. (6) The natural history of most untreated giant aneurysms is extremely dismal. The literature contains very few cases of complete spontaneous occlusion of partially thrombosed giant BA aneurysms. (1,12,13) However, during recent decades, good outcomes after the treatment of ruptured and unruptured pediatric aneurysms have increased.(5)