Shrestha M, Basnet S, Shrestha PS.
Department of Child Health, Tribhuvan University Teaching Hospital, Kathmandu, Nepal.
ADDRESS FOR CORRESPONDENCE
Dr Merina Shreshta, Lecturer Department of Child Health, Tribhuvan University of Teaching Hospital, Maharajgung, Kathmandu, Nepal.
Email: shresthamerina@hotmail.com | | Abstract | Objective: To assess the efficacy of a liquid crystal device (ThermoSpot) in detecting neonatal hypothermia.
Methods: It was a hospital based, cross-sectional study. The study included 300 newborn babies born in our hospital. These babies were assessed thrice in first 24 hours of life i.e. within 4 hour, 4- 12 hours and 12-24 hours. Axillary temperature of these babies was recorded by low-reading glass in mercury thermometer and colour in the ThermoSpot was also noted and compared to analyze the sensitivity and specificity of ThermoSpot in detecting neonatal hypothermia.
Results: In the 1st assessment, out of 300, 96.3% babies had hypothermia out of which 73.7% babies had mild and 26.3% babies had moderate hypothermia. In the 2nd assessment, out of 294 babies, 72.8% babies were hypothermic of which 93% had mild and only 7% had moderate hypothermia. In the 3rd assessment, out of 294 babies, 47.75 %babies were hypothermic of which 99.3% had mild and 0.7% had moderate hypothermia. Sensitivity and Specificity of ThermoSpot in detecting moderate hypothermia was found to be 97.8% and 99.8% respectively. The positive predictive value of ThermoSpot in detecting moderate hypothermia was 98.9 %. The negative predictive value was 99.63%.
Conclusion: Liquid crystal device "ThermoSpot"; can be used with ease even for continuous monitoring of temperature. | | | | Keywords | | Newborn, Hypothermia, Liquid crystal device | | | | Introduction | Newborn babies are prone to hypothermia because of their limited ability to generate and conserve heat. The condition may occur later too, during bathing or on a cold night, if measures to keep the baby warm are inadequate. Neonatal hypothermia is classified as cold stress, moderate and severe hypothermia with temperature of 36.0 - 36.4⁰C, 32 - 35.9⁰C and below 32⁰C respectively. (1) Prolonged hypothermia is associated with impaired growth (2) and may make the newborn more vulnerable to infections. (3) It is one of the important factors related to mortality among nursery admissions as well. (4) Tafari, in Addis Ababa, found hypothermia in 53% of neonatal unit admissions and there was linear increase in mortality with decreasing temperature at admission. Fifty nine percent of those with temperature < 36⁰C died compared to 15% with temperature ≥ 360C. (5) Moreover, hypothermia, even if moderate, is associated with an increased risk of death in low birth weight (LBW) newborns. Sick or LBW neonates admitted to neonatal units with hypothermia are more likely to die than those admitted with normal temperatures.(1,5-7) So if early interventions are not carried out for newborn babies to keep them warm, they may become severely hypothermic and may present with one or many complications like thrombocytopenia, disseminated intravascular coagulation, pulmonary hemorrhage, renal failure, seizures, patent ductus arteriosus, intracranial hemorrhage, necrotizing enterocolitis and gastrointestinal perforation etc.(8) To overcome these complications monitoring the temperature of newborn is essential.
In developed countries, digital thermometer, ear thermometer, a single use thermometer (tempa-DOT) are commonly used. But these types of thermometers are more sophisticated to use and are not easily available. In developing countries, a mercury-in-glass thermometer is generally used (1). However, rectal temperature measurement carries a small risk of bowel perforation and cross infection. (9-11) This conventional thermometer also fails to detect hypothermia below 35⁰C and low reading rectal thermometers are not easily available as well as not easy to use in the community and home environment. The reading takes some effort and practice. Moreover, mercury thermometers are an environmental hazard as vigorous shaking prior to and after checking the temperature may cause it to break and mercury to spill over. Many countries are even starting to ban the routine use of these mercury thermometers in health care facilities. (14) Lastly, thermometers provide us an idea of the body temperature only at a particular point of time that is when it is checked. Therefore, liquid crystal device could be used to detect neonatal hypothermia as even illiterate mothers themselves can easily identify the color change in the device and the device is affordable in developing countries like ours. So this liquid crystal device could be added to the delivery kit for detecting neonatal hypothermia in the community level.
This study was conducted in an attempt to verify the reliability of liquid crystal device in detecting hypothermia in newborns and as such help the community level workers and mothers/caretakers to identify hypothermia easily and take appropriate actions to prevent unforeseen complications due to hypothermia on time. This Liquid crystal temperature indicator called Thermospot was developed by Camborne Consultants of UK, which is a sticky black disc (12mm in diameter). This device can be placed over the axilla, hypochondrium or just lateral to the suprasternal region. Provided the newborn baby's temperature is 35.5⁰C or more, the disc changes to green. If, however, the temperature falls below 35.5⁰C the disc reverts back to black. The device adheres to the skin firmly and can last up to 7-10 days, thus providing continuous temperature monitoring. Even it comes off it can be re-applied with transparent tape. The changes that happen on the device can be explained to mothers or caretakers and thereby appropriate action could be taken. (15) | | | | Methods & Materials | It was a hospital based cross sectional study conducted in maternity ward, Tribhuban University Teaching Hospital, Maharajgunj, Kathmandu from 2004, Nov 20 to 2005, Apr 24. Out of 1722 newborn babies born during study period, 300 newborn babies less than 4 hours old and kept in postnatal ward were included in the study. Those babies who were admitted in the neonatal nursery, of very low birth weight, had low APGAR score (less than 7/10 at 5 minutes), who were getting antibiotics and had congenital anomalies were excluded from the study. Each baby was thoroughly examined, partially undressed, three times in first 24 hours of life. The first assessment was done within 4 hours; second assessment between 4 to 12 hours & third assessment between 12 and 24 hours of life and findings were recorded according to the proforma prepared for the study.
In the first assessment, the liquid crystal device was stuck on the top of the skin of the baby over right hypochondriac region, just below costal margin at mid clavicular line. This area was chosen, as it is the easiest place to observe the color change in the device without undressing the baby clad in the traditional Nepali newborn dress 'bahule bhoto'. The color change in ThermoSpot was observed 10 minutes after sticking the device in the first assessment and subsequently in 2nd and 3rd assessment. During each assessment, the temperature was also assessed using a thermometer placed in the axilla for 5 minutes. Before starting the study, all the staffs of neonatal nursery and maternity ward were briefed about the study. The color change in the ThermoSpot was demonstrated by sticking the "black" ThermosSpot to the outside wall of a drinking glass, half-filled with cold water and hot water was gradually added to it. When the temperature rose, the black disc turned green. Mothers/caretakers were also demonstrated the color change in the device and they were asked to notice the color change in the device every time they change the wet nappy and also to see whether the device is in its place or not and if they notice black color or if the device has fallen, then to inform on-duty doctor/nurse. During the study whenever the babies were found to have black disc and moderately hypothermic with other signs of hypothermia (like lethargy, cyanosis) they were transferred to neonatal nursery and appropriately managed. Those babies who were transferred to nursery were excluded in the subsequent assessments. All the datas collected were processed with computer aid using SPSS programme and sensitivity and specificity of the non-invasive liquid crystal thermometer was calculated. | | | | Results | Of the 300 babies, 56.3 %were male and 43.7 % were female. There were two sets of twins in the study population. 5.3 % babies were preterm. The mean birth weight of these babies was 3120.75±466 grams. Figure 1 shows the incidence of hypothermia in 3 assessments i.e. within 4 hours, 4-12 hours and 12-24 hours of life and also the distribution of mild and moderate hypothermia. This figure clearly shows the decrease in incidence of hypothermia in subsequent assessments with increase in the percentage of mild hypothermia and decrease in the percentage of moderate hypothermia. Total of 888 readings were taken during all three assessments. Out of these readings, ThermoSpot was black in 91 (10.3 %) occasions and 90 (97.8%) times it correlated with moderate hypothermia while 797(89.7%) times ThermoSpot remained green. Only on 2 (2.2%) occasions, when temperatures recorded were < 35.50⁰C, the ThermoSpot remained green. For detection of moderate hypothermia, ThermoSpot was found to be 97.8 % sensitive and 99.8% specific. The positive predictive value of ThermoSpot in detecting moderate hypothermia was 98.9 %. The negative predictive value was 99.63%. The finding was statistically highly significant (p = 0.001). (Table No: 1)
Fig 1: Incidence of Hypothermia in Each Assessment
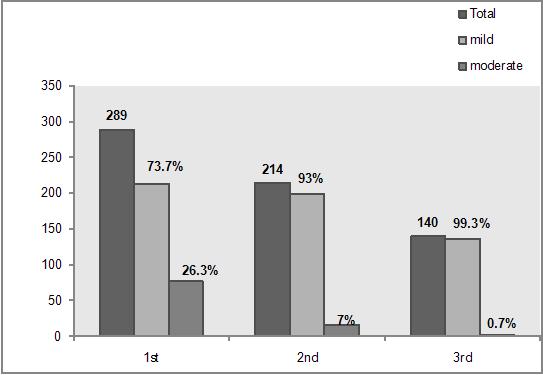
Table 1: Detection of hypothermia using ThermoSpot as compared to axillary temperature
|
Axillary temperature in Celsius |
Total |
| < 35.5 |
35.5 - 36.5 |
= 36.5 |
| Thermospot Reading: |
Yes |
90 (97.8 %) |
1 (1.1 %) |
0 |
91 |
| Black |
No |
2 (0.3 %) |
550 (69 %) |
245 (30.7%) |
797 |
| Total |
92 |
551 |
245 |
888 |
| | | | Discussion | The main objective of this study was to see the effectiveness of a liquid crystal indicator, the "ThermoSpot" in detecting neonatal hypothermia and its correlation with axillary temperature. There are many studies showing good correlation between axillary temperature and the rectal temperature in the detection of hypothermia. (16-17) The axillary temperature recording was therefore taken as a gold standard in the detection of hypothermia for the present study. The incidence of hypothermia in the postnatal ward was found to be quite significant. Of the babies, 96.3 % were hypothermic in the first 4 hours followed by 72.8% between 4 to 12 hours and 47.7 % between 12 to 24 hours of which in the first 4 hours, 71 % and 25.3% of the babies had mild and moderate hypothermia respectively. In the 2nd assessment, 93% of the babies were mildly hypothermic and 7% were moderately hypothermic. In 3rd assessment, 99.3% of the babies were mildly and 0.7% babies were moderately hypothermic. There was a decreasing incidence of moderate hypothermia but with more babies in cold stress at 24 hours. In the study conducted by Johanson et al (18) at Prasuti Griha Maternity Hospital in Nepal in 1988, in the cold season of mid February, 85 % of babies were hypothermic at 2 hours of birth and nearly 50% were still moderately hypothermic at 24 hours. The findings are different from the current study as only 0.7% of the babies were moderately hypothermic at 24 hours. In Johanson's study, the incidence of hypothermia quoted above was in those babies in whom no interventions were carried out after the detection of hypothermia (the observation group) but the lower incidence of moderate hypothermia in the present study might be due to the reason that counseling of mothers/caretakers and early interventions like keeping babies close to mothers/caretakers body, keeping them in sunlight and at times even provision of room heaters to keep these newborn babies warm were carried out when hypothermia was detected. In another study conducted by Ellis et al (19) in 1993-1994 at Prasuti Griha maternity hospital, 72% of the neonates had hypothermia during first 8 hours of life, 31% at 8-16 hours of life and 15% at 16-24 hours of life. Although this study too shows a declining trend in the incidence of hypothermia with increasing age of the babies in hours the findings of this study could not be compared as the assessment of hypothermia was done at different intervals i.e. within 4 hours, 4 to 12 hours and 12 to 24 hours of life in the present study.
For prevention of various complications of neonatal hypothermia (8), early detection is necessary. Hypothermia can be detected by measuring temperature using glass-in- mercury thermometers or simpler methods like liquid crystal device In the present study, liquid crystal device was compared with axillary temperature recording in detecting neonatal hypothermia. It was found that the device was 97.8% sensitive and 98.9% specific in detecting moderate hypothermia. The present study thus is comparable with the study done by Valadezz et al (20) at John Hopkins School of Hygiene and Public Health in Maryland, USA. He found that the liquid crystal device had a sensitivity of 100% and specificity of 92%. Similarly, Morrice et al (21) found that the device is 100% sensitive in detecting neonatal hypothermia. Another study done by Manandhar et al (22) found liquid crystal thermometer to be 83% sensitive and 92% specific in detecting neonatal hypothermia. The sensitivity of the device is low as compared to the present study as this might be due to small sample size including only 76 newborns as compared to 300 newborns in the current study. Liquid crystal device was able to detect hypothermia not only in the ward but also in the patients in intensive care unit which was proven in the study done by Chernishev et al (21). On comparing axillary temperature recordings with the liquid crystal device, he found the device to be as good in detecting moderate hypothermia with 'p' value of <0.05 which is comparable to the present study. | | | | Conclusion | | Neonatal hypothermia is still a common problem even in hospitals. Hence liquid crystal device could be used for continuous monitoring so as to prevent hypothermia as it is 97.8% sensitive and 99.8% specific in detecting hypothermia with temperature of <35.5oC. However, this device cannot detect the newborn babies in cold stress. Mercury in glass thermometer remains the gold standard. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- WHO. Thermal protection of the newborn: a practical guide. In: maternal and newborn Health and Safe Motherhood program. Division of Reproductive health, World health Organization, Geneva, 1997.
- Glass L, Silverman WA, Sinclair JC. Effect of the thermal environment on cold resistance and growth of small infants after first week of life. Pediatrics 1968; 41: 1033-1046. [PubMed]
- Lyon A, Pikaar M, Badger P, McIntosh N. Temperature control in very low birthweight infants during first five days of life. Arch Dis Child Fetal Neonatal Ed. 1997; 76: F47-F50. [CrossRef]
- Rennie JM, Roberton NRC. Temperature control and its disorder. Textbook of Neonatology, 3rd ed. Churchill Livingston. 1999: 289-303.
- Tafari N, Sterky G, Tunell R eds. Breathing and warmth at birth. Epidemiological aspects. Sarec Report.1985: 53-58. [PubMed]
- Ji XC, Zhu CY and Pang RY. Epidemiological study on hypothermia in newborns. Chin Med J (Engl). 1993; 106: 428-432.
- Daga AS, Daga SR, Patole SK. Determinants of death among admissions to intensive care unit for newborns. J Trop Pediatr. 1991; 37: 53-56. [CrossRef]
- Kaplan M, Eidelman AI. Improved prognosis in severely hypothermic newborn infants treated by rapid rewarming. J Pediatr. 1984; 105: 470-474. [CrossRef]
- Im SW, Chow K, Chau PY. Rectal thermometer mediated cross-infection with Salmonella wandsworth in a paediatric ward. J Hosp Infect. 1981; 2: 171-174. [CrossRef]
- Greenbaum EI, Carson M, Kincannon WN, O'Loughlin BJ. Rectal thermometer-induced pneumoperitoneum in the newborn. Report of two cases. Pediatrics. 1969; 44: 539-542. [PubMed]
- Horwitz MA, Bennett JV. Nursery outbreak of peritonitis with pneumoperitoneum probably caused by thermometer-induced rectal perforation. Am J Epidemiol. 1976; 104: 632-644. [CrossRef]
- Akinbami FO, Sowunmi A. Body temperature in the Nigerian neonate--comparison of axillary and rectal temperatures. Afr J Med Med Sci. 1991; 20: 49-52. [PubMed]
- Chaturvedi D, Vilhekar KY, Chaturvedi P, Bharambe MS. Comparison of axillary temperature with rectal or oral temperature and determination of optimum placement time in children. Indian Pediatr. 2004; 41: 600-603. [PubMed]
- Blumenthal I. Should we ban the mercury thermometer? Discussion paper. J R Soc Med. 1992; 85: 553-55. [PubMed] [PMC free article]
- N Kennedy, Lilian Gondwe, DC Morley. Temperature monitoring with ThermoSpots in Malawi Lancet 2000: 355: 659-660.
- Akinbami FO, Sowunmi A. Body temperature in the Nigerian neonate--comparison of axillary and rectal temperatures. Afr J Med Med Sci. 1991; 20: 49-52. [PubMed]
- Sarman I, Can G, Tunell R. Rewarming preterm infants on a heated, water filled mattress. Arch Dis Child. 1989; 64: 687-692. [CrossRef]
- Johanson RB, Spencer SA, Rolfe P, Jones P, Malla DS. Effect of post-delivery care on neonatal body temperature. Acta Paediatr. 1992; 81: 859-863. [CrossRef]
- Ellis M, Manandhar N, Shakya U, Manandhar DS, Fawdry A, Costello AM. Postnatal hypothermia and cold stress among newborn infants monitored by continuous ambulatory recording. Arch Dis Child Fetal Neonatal Ed. 1996; 75: F42-F45. [CrossRef]
- Valadez JJ, Elmore-Meegan M, Morley D. Comparing liquid crystal thermometer readings and mercury thermometer readings of infants and children in a traditional African setting. Implications for community-based health. Trop Geogr Med. 1995; 47: 130-133. [PubMed]
- Thermospot. Available at URL: http://maternova.net/images/maternova/thermospot.pdf. Accessed on 12th June 2010.
- Manandhar N, Ellis M, Manandhar DS, Morley D, de L Costello AM. Liquid crystal thermometry for the detection of neonatal hypothermia in Nepal. J Trop Pediatr. 1998; 44: 15-17. [CrossRef]
|
| Cite this article as: | | M S, S B, PS S. Comparison of Liquid Crystal Device -ThermoSpot with Low Reading Axillary Thermometer in Detecting Neonatal Hypothermia. Pediatr Oncall J. 2010;7: 67-70. |
|