Girija Mohan, Krishnan C, Sheeja Sugunan, Sathesh Kumar K.
Department of Pediatrics, Govt T D Medical College, Alappuzha.
ADDRESS FOR CORRESPONDENCE
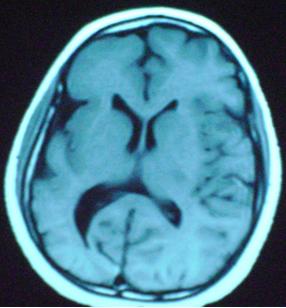
Dr Girija Mohan, Professor & HOD, Dept of Pediatrics, Govt TD Medical College, Alappuzha. | | Keywords | | Hemiatrophy, Seizure | | | A 9 years old deaf-mute girl presented with recurrent seizures, left hemiparesis and left hemiatrophy. The patient was the third child of non consanguineous parents with no significant family history. The child was born prematurely at 33 wks of gestation with a birth weight of 1.8kg .There was no birth asphyxia but was in Neonatal Intensive Care Unit for 10 days for low birth weight care. She had global developmental delay and was noticed to be deaf-mute from early infancy. She developed generalized tonic clonic convulsions from the age of 4 years. Even regular treatment with multiple anti-epileptic drugs failed to control seizures adequately. On examination the child had microcephaly, facial asymmetry and marked hypoplasia of left side of body. There was left hemiparesis with grade IV power and brisk deep tendon reflexes. There was moderate mental retardation also. MRI brain showed atrophy of left cerebral hemisphere, dilatation of the ipsilateral ventricle, widening of right sylvian fissure and ipsilateral sulci. Right frontal sinus was enlarged. (Fig 1) A CT scan done during early childhood (film was lost) showed calvareal thickening in addition.
Figure 1: MRI brain showing atrophy of right cerebral hemisphere with dilated ipsilateral ventricle and widened sylvian fissure.
Dyke-Davidoff-Masson Syndrome (DDMS) is characterized by contralateral hemiplegia, seizures, facial asymmetry, varying degree of atrophy of one side of body and mental retardation. (1)The diagnosis is essentially made from the characteristic radiologic features like cerebral hemi hypoplasia, ipsilateral osseous hypertrophy and hyper pneumatization of sinuses. (1,2) DDMS was first described by Dyke, Davidoff and Masson in 1933 in a series of 9 patients with hemiparesis, seizure, facial asymmetry and mental retardation. The skull x-ray and pneumoencephalogram of these patients showed thickening of calvarium and dilatation of ipsilateral frontal and ethmoid sinuses. There was also elevation of the greater wing of sphenoid and petrous ridge and upward tilting of planum - sphenoidale .(2) In 1939 Alpers and Dear classified the disease into primary (congenital) type and secondary (acquired) type .(3) Congenital type becomes symptomatic in perinatal period or during infancy. Vascular occlusion during gestational or neonatal period involving middle cerebral artery (MCA) territory, unilateral cerebral artery circulation anomalies, coarctation of mid aortic arch, mesencephalon hypoplasia and wallerian degeneration has been postulated as the etiology for this .(4,5) In acquired type causative factors are trauma, infection, ischemia or hemorrhage .(6) Age of presentation depends on time of insult. Characteristic whole features may evolve only during adolescence. Other associated findings described are sensory loss, speech and language disorders, learning disability and psychiatric manifestations like schizophrenia. Prognosis is better if hemiparesis occurs after 2 years and in the absence of intractable seizures. Children with intractable, disabling seizure may be candidates for hemispherectomy, which is successful in 85% of selected cases .(7) Present case seems to be infantile type, as the symptoms started in early infancy and there is no definite history of central nervous system insult in the post neonatal period.
Contributors: GM diagnosed the case and supervised the management, KC drafted the manuscript, SS and S were involved in patient management and review of literature. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Tasdemir HA, Incesu L, Yazicioglu AK, Belet U, Gungor L. Dyke-Davidoff-Masson syndrome. Clin Imaging. 2002; 26: 13-17. [CrossRef]
- Dyke CG, Davidoff LM, Masson CB. Cerebral Hemiatrophy and homolateral hypertrophy of the skull and sinuses. Surg Gynecol Obstet 1933; 57: 588-600.
- Alpers BJ, Dear RB. Hemiatrophy of the brain. J Nerv Ment Dis. 1939; 89: 653-651.
- Teal JS, Rumbaugh CL, Bergeron RT, Segall HD. Congenital absence of the internal carotid artery associated with cerebral hemiatrophy, absence of the external carotid artery, and persistence of the stapedial artery. Am J Roentgenol Radium Ther Nucl Med. 1973; 118: 534-545. [CrossRef] [PubMed]
- Parker JC Jr, Gaede JT. Occurrence of vascular anomalies in unilateral cerebral hypoplasia. "Cerebral hemiatrophy". Arch Pathol. 1970; 90:265-270. [PubMed]
- Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging. 1992; 16: 93-97. [CrossRef]
- Narain NP, Kumar R, Narain B. Dyke-Davidoff-Masson syndrome. Indian Pediatr. 2008; 45: 927-928. [PubMed]
|
| Cite this article as: | | Mohan G, C K, Sugunan S, K S K. Dyke Davidoff Masson Syndrome. Pediatr Oncall J. 2010;7: 116. |
|