Shashidhar A, J Harish, S R Keshavamurthy.
Department of Pediatrics, Kempegowda Institute of Medical sciences, Bangalore, India.
ADDRESS FOR CORRESPONDENCE
Dr Shashidhar, #114, KIMS Mens Hostel, Near BDA Complex, Banashankari 2nd stage, Bangalore-70, India.
Email: shashiishere@gmail.com | | Abstract | Objective: To estimate the prevalence, pattern, and correlates of smoking amongst high school children in Bangalore South and to assess their knowledge and attitude towards smoking.
Methods: A cross-sectional study was conducted in 2 randomly selected schools in Bangalore South.
A total of 501 students participated in the study in the age group of 12-17yrs. The knowledge attitude and practice of smoking were assessed using a pre-designed questionnaire.
Results: Prevalence of smoking was 6.8%. Smoking was predominantly a male feature and about half were occasional smokers (once in 3 months). Peer influence was cited as the most common initiating factor and the 1st puff was taken most commonly at mean age of 13 yrs. Majority of non-smokers (88%) cited "bad for health" as the primary reason for not smoking. More than half the children had a smoker in the house and about 40% had no idea about dangers of smoking. Majority of participants had never been taught about smoking either in school or at homes and more than half obtained information about smoking from TV.
Conclusion: The prevalence obtained correlates with similar studies in India and highlights smoking as a major health and social issue in adolescents. The results clearly indicate major lacunae not only in current educational system but also in parental upbringing not giving worthy importance to smoking and its health hazards. The need of the hour is to target and focus interventions through comprehensive programmes aimed at children, school authorities, parents and policy makers. | | | | Keywords | | Smoking; Prevalence; India; School health services; adolescent | | | | Introduction | | Tobacco is the single largest cause of death and disability worldwide. (1) Globally everyday about 80,000-1,00,000 youth initiate smoking, most of them are from developing countries (2). About one-fifth of all worldwide deaths attributed to tobacco occur in India (3). It was estimated in 1999-2001 that 5500 adolescents start tobacco use everyday in India joining the 4 million under 15 children who already use it regularly (4). The most susceptible time for initiation of tobacco use in India is adolescence and early adulthood ages 15-24 yrs (5). Of 1000 teenagers who smoke today, 500 will eventually die of tobacco related diseases, 250 in their middle age and 250 in their old age(6). Tobacco use in adolescents has been called a "paediatric epidemic" because of increasing level of its use and dire public health implications.(7) | | | | Methods & Materials | A cross-sectional study was done among high school children in 2 schools in Bangalore South urban area during July-August 2009. One was a government school and other was a private school catering for children belonging to low to middle socioeconomic status. Both schools were providing co-education in English medium. A verbal consent of the Principals of the schools selected for the study was taken, prior to starting the study. Informed oral consent was taken from all the participants. All participants were reassured about their anonymity during the administration of the questionnaire. Data were collected by pre-tested anonymous self-administered questionnaires in the classroom by one of the investigators. All students in the selected class divisions were eligible to participate. Non-response was due to absence in the class. Teachers were asked to leave the classroom during survey administration. The questionnaire covered five broad categories: (1) demographics and personal information; (2) knowledge and attitudes, knowledge of health effects of smoking, and attitudes towards tobacco use; (3) tobacco use-by the participant and by others in his/her home and community; (4) source of smoking related information; and (5) passive smoke exposure.
Any doubts about the questionnaire were clarified to the children by the investigator. Most of the questions required the pupil just to tick the best suited answer.
Statistical Methods: Descriptive statistical analysis has been carried out. Results on continuous measurements are presented on Mean + SD (Min-Max) and results on categorical measurements are presented in number (%). Significance is assessed at 5 % level of significance.
| | | | Results | A total of 501 high school children took part in the study of which 34 were smokers (6.8%) of which 2 (2.4%) were 13 years old, 15 (7.4%) were 13 years old, 15 (7.4%) were 14 years old, 9 (5.8%) were 15 years old and 8 (16%) were 16 years old. The 1st puff was taken most commonly at a mean age of 13.1 ± 1.4 years. Two children (5.9%) had the 1st puff at 10 years of age, 3 children (8.8%) had 1st puff at 11 years of age, 9 children (26.5%) had first puff at 12 years of age, 6 children (17.6%) had first puff at 13 years of age, 8 children (23.5%) had first puff at 14 years of age and 6 children (17.6%) had first puff at 15 years of age.
Male:Female ratio was 264:237. Smoking was predominantly a male feature and prevalence was about 9 times higher in males. Thirty-one (11.7%) boys smoked as compared to only 3 (1.3%) girls. (p=0.002). About half were occasional smokers (once in 3 months).
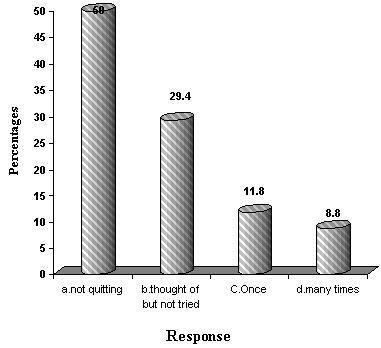
Peer influence was cited as the most common initiating factor for smoking. The commonest reasons why they started smoking are depicted in Fig. 1. Twenty children (58.8%) stated that they continued to smoke because it is stylish, 6 (17.6%) stated that it relieves tension, 4 (11.8%) stated that it is pleasurable, 3 children (8.8%) stated that they smoked because most of their friends smoked and one stated that he smoked because he is grown up. Half of them had not thought of quitting. (Figure 2)
Fig. 1: What was the most important thing that made you start smoking?
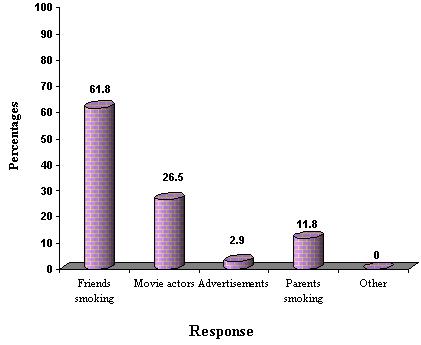
Figure 2: Have you tried quitting smoking?
Though majority of non-smokers (88%) cited "bad for health" as the primary reason for not smoking, 48.5% were not sure about harmfulness of smoking. (Table 1).
Table 1: Why have you not started smoking?
| Reason for not smoking |
Number
(n=501)
|
% |
| bad for health |
444 |
88.6 |
| parents do not allow |
30 |
5.9 |
| no money |
6 |
1.2 |
| not fashionable |
2 |
0.3 |
| other (specify) |
- |
- |
| No response |
31 |
6.2 |
| Effects of smoking |
|
|
| Harmful |
258 |
51.5 |
| OK |
21 |
4.2 |
| Healthy |
14 |
2.8 |
| Don't know |
205 |
40.9 |
More than half the children had a smoker in the house, (70% in case of smokers) most often the father. (Table 2)
Table 2: Does anyone smoke in your house?
| Response |
Number (n=501) |
% |
| Brother |
26 |
5.2 |
| Father |
179 |
35.7 |
| Cousin |
15 |
2.9 |
| Other relative |
69 |
13.8 |
| none |
218 |
43.5 |
Majority of participants had never been taught about smoking either in school (83.4%) or at homes (81.6%). The best source of smoking-related information was found to be television according more than half the participants. (Table 3)
Table 3: Best source for information on smoking
| Response |
Number (n = 501) |
% |
| TV |
294 |
58.7 |
| Newspaper/magazines |
107 |
21.4 |
| Internet |
59 |
11.8 |
| Friends |
86 |
17.2 |
| Parents |
50 |
9.9 |
| | | | Discussion | The prevalence of smoking at 6.8% is slightly higher than that reported by Gururaj et al (5.1%) in GYTS-Karnataka but lower against the national average of 17.5% (8). The prevalence was found to be highest at 16 yrs in our study. Female smokers constituted only about 1.3% of the children. This may be due to the fact that the schools were mainly catering for non-affluent urban children. The influence of peers found in this study is similar to research in India and elsewhere. In their recent synthesis, the US group of Jacobsson and colleagues (10) concluded that peer influence was the strongest predictor of smoking initiation. The amount of information gained through school curricula and parents was negligible and students were mainly dependent on mass media for such information. This study thus indicates the urgent need for including smoking-related information in the school curricula before the mean age of initiation (13yrs). Enabling teachers to educate the young impressionable minds regarding life style disorders should be a cornerstone activity in preventing the establishment of life style disorders like tobacco and alcohol use within the community. Parents should also be educated to speak to the teenagers more often in this regard. A comprehensive tobacco control programme that goes beyond the communication of health dangers which includes the community and school is needed to curb adolescent smoking and to provide healthy young citizens for the nation.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- World Health Organisation (WHO). WHO program on tobacco on health. Geneva. 1995.
- Jha P, Chaloupka FJ. Curbing the Epidemic: Governments and the Economics of tobacco Control. Washington D.C, The World Bank, 1999.
- World Health Organization (WHO). Making a difference World Health Report, Geneva. 1999.
- Reddy KS, Gupta PC (eds). Report on Tobacco Control in India. Ministry of Health and Family Welfare, New Delhi, Government of India, 2004.
- National Sample Survey Organization (NSS). A note on consumption of tobacco in India, NSS 50th round (1993-1994). Sarvekshana: A Journal of the National Sample Survey Organization 1998; 21: 69-100.
- Peto R. Education and debate. Smoking and death: the past 40 years and the next 40. BMJ. 1994; 309: 937-939. [CrossRef]
- Perry CL, Eriksen MP, Giovino G. Tobacco use: A pediatric epidemic. Tob Control. 1994; 3: 97-98. [CrossRef]
- Gururaj G, Girish N. Tobacco Use amongst Children in Karnataka. Indian J Pediatr. 2007; 74: 1095-1098. [CrossRef] [PubMed]
- Gupta PC, Ray CS. Smokeless tobacco and health in India and South Asia. Respirology. 2003; 8: 419-431. [CrossRef]
- Jacobsson PD, Lantz PM, Warner KE, Wasserman J, Pollack HA, Ahlstrom AK. Combating Teen Smoking. Research and Policy Strategies. Ann Arbor MI: 2001. [CrossRef]
|
| Cite this article as: | | A S, Harish J, Keshavamurthy S R. Adolescent Smoking - A Study of Knowledge, Attitude and Practice in High School Children. Pediatr Oncall J. 2011;8: 1-3. |
|