H Daish, A Gite, S Mukherjee.
Department of Paediatrics, Basildon University Hospital, Essex, UK.
ADDRESS FOR CORRESPONDENCE
Dr Gite A, 22 Mander Way, Cambridge, CB1 7SF, UK.
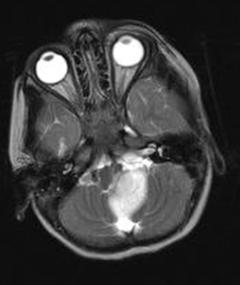
Email: gite_amitabh@yahoo.com | | Abstract | | Although isolated torticollis is a known presenting feature of posterior fossa tumors, it is rare for it to present in isolation for a very prolonged period of time. Posterior fossa tumors are reported to occur most commonly in children aged 6-8 years. We present a case of astrocytoma in a 2 1/2 year old girl who presented with isolated, non-progressive torticollis for 2 years. We demonstrate the importance of considering the diagnosis of posterior fossa tumor as the underlying cause of torticollis, even if the child is very young and the symptoms not progressing. | | | | Introduction | | Torticollis has a wide variety of underlying causes, ranging from benign to life-threatening (1). Posterior fossa tumors are an uncommon cause of torticollis and instead usually present with features of raised intracranial pressure (2). When torticollis is the sole presenting feature of posterior fossa tumors, it usually remains as an isolated symptom only for a short period of time (3). We report here a 2 1/2 year old girl who presented with a 2 year history of isolated non-progressive torticollis secondary to posterior fossa tumor. | | | | Case Report | A 2 1/2 year old girl was referred, for cosmetic reasons, for torticollis present since the age of 6 months. The General Practitioner initially diagnosed this as congenital torticollis. She was otherwise asymptomatic, had no significant past medical history and no history of trauma. Her torticollis had neither improved nor worsened over the last 2 years, was continuously present and always to the left side. On examination she was noted to have left sided torticollis with restricted movement to the right; passive movement did not cause any discomfort. On examination of the nervous system, cranial nerves, tone, plantar reflexes and gait were normal. No focal neurological signs were present. She had normal vision and strabismus was not present. There were no palpable neck masses. The rest of the systemic examination found no other abnormalities. Her developmental milestones were normal and she was on the 50th centiles for height and weight. Due to persistent torticollis, an MRI of her brain and spinal cord was requested which showed a well-demarcated tumor (23x33mm) between the left cerebellar hemisphere and medulla. The medulla oblongata was pushed anteriorly and to the right side. The ventricles were normal (Fig 1).
Fig 1. MRI brain showing posterior fossa tumor
She underwent debulking surgery and the histology showed low grade (WHO 1) pilocytic astrocytoma. Technically difficult surgery prevented complete tumor resection and was complicated by post-operative bulbar palsy with swallowing difficulty and aspiration pneumonia. Adjuvant chemotherapy was commenced. | | | | Discussion | Torticollis may be either congenital or acquired (1). Congenital torticollis tends to have its onset within the first few weeks of life, the commonest cause being intrauterine sternomastoid muscle contracture. Acquired causes range from benign to life-threatening and include cervical adenitis, retropharyngeal abscess, benign paroxysmal torticollis, posterior fossa tumors and trauma. (1) In this case, torticollis was first noticed at 6 months of age, suggesting an acquired cause.
Pilocytic astrocytoma is usually a slow-growing childhood tumor. The most common clinical features are vomiting, ataxia, headaches and focal neurological signs, depending on the site. (2) Torticollis secondary to posterior fossa tumors is usually associated with other symptoms. However, there have been several reports of isolated torticollis as the presenting feature of posterior fossa tumors prior to development of other symptoms. (2-4) This makes the clinical suspicion of posterior fossa tumors difficult. Turgut et al report a high incidence of initial misdiagnosis of torticollis as the first presentation of posterior fossa tumours. (3) Common misdiagnoses include behavioral, ophthalmological, psychological and cervical spine problems. (2)
A report of 23 children with acquired torticollis due to posterior fossa tumors found that the longest duration for this symptom to remain in isolation was 4 months. (3) The case we have reported, however, is of a much more insidious course with a 2 year history of isolated, unprogressive, torticollis as the presentation. The child presented here was first symptomatic at 6 months of age. This is an unusual age for presentation of posterior fossa astrocytomas; one report presents the mean age at presentation of these tumors as 6.6 years. (5) Another presents the mean age at presentation of posterior fossa tumors as 8.1 years, (2) thus making a posterior fossa tumor a less likely underlying cause of torticollis presenting in infancy. However, despite posterior fossa tumors usually presenting in older children, this case highlights the need to consider this diagnosis even if the onset of torticollis is within the first few years of life. | | | | Conclusion | | In conclusion, torticollis may be the presentation of a wide variety of underlying conditions. This report emphasizes the importance of carefully considering the need for investigation of torticollis to rule out serious causes, even if torticollis is the only clinical feature. Similarly, investigation needs consideration even if there appears to be no progression of the torticollis over a prolonged period of time. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Spiegel DA, Hosalkar HS, Dormans JP, Drommond DS. The neck. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia, Saunders Elsevier; 2007: 2822.
- Dorner L, Fritsch M, Stark A, Mehdorn H. Posterior fossa tumors in children: how long does it take to establish the diagnosis? Childs Nerv Syst 2007; 23: 887-890. [CrossRef]
- Turgut M, Akalan N, Bertan V, Erbengi A, Eryilmaz M. Acquired torticollis as the only presenting symptoms in children with posterior fossa tumors. Child's Nerv Syst 1995; 11: 86-88. [CrossRef]
- Kumandas S, Per H, Gumus H, Tucer B, Yikilmaz A, Kontas O, et al. Torticollis secondary to posterior fossa and cervical spinal cord tumors: report of five cases and literature review. Neurosurg Rev 2006; 29:333-338. [CrossRef]
- O'Brien DF, Caird J, Kennedy M, Roberts GA, Marks JC, Allcutt DA.Posterior fossa tumors in childhood: evaluation of presenting clinical features. Ir med J 2001; 94:52-53. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2012.36
|
| Cite this article as: | | Daish H, Gite A, Mukherjee S. A RARE PRESENTATION OF A COMMON ASSOCIATION. Pediatr Oncall J. 2012;9: 43-44. doi: 10.7199/ped.oncall.2012.36 |
|