Bhavana Lakhkar1, Bhushan Lakhkar2, Abhilasha1.
1Department of Pediatrics, Jawaharlal Nehru Medical College, Sawangi Meghe, Wardha, India,
2Department of Radiology, Jawaharlal Nehru Medical College, Sawangi Meghe, Wardha, India.
ADDRESS FOR CORRESPONDENCE
Dr. Bhavana Lakhkar, Department of Paediatrics, AVBRH, Sawangi (Meghe), Wardha 442002, India.
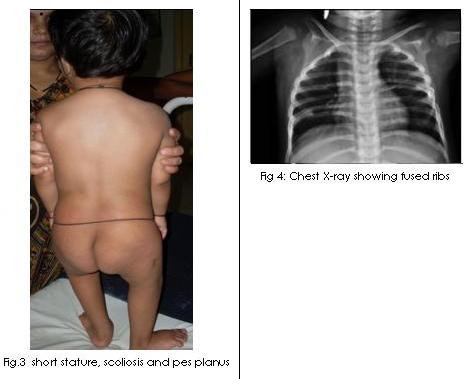
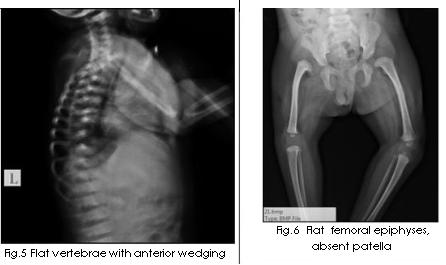
Email: blakhkar@yahoo.co.in | A two year old child was admitted to our hospital for surgical intervention of cleft palate. On general physical examination, the child was found to have micrognathia, posteriorly placed tongue and midline cleft of soft palate with a rounded contour (Fig.1 & 2). So, a diagnosis of Pierre Robin sequence was made. On further detailed examination, we noticed that the child had short stature (length of 75 cm, < 5th percentile), low set ears, clinodactyly, exaggerated lumbar lordosis, mild scoliosis, pes planus, genu valgus (Fig. 3) and waddling gait. X ray spine, pelvis, knee joint, ankle joint, foot and chest was taken which showed the following features: flat vertebrae, anterior wedging of vertebrae, flat irregular femoral epiphyses, absent patella, underdeveloped distal tibial epiphyses and fused ribs (Fig. 4, 5 & 6). Ophthalmologic evaluation revealed myopia and astigmatism. Hearing assessment showed bilateral moderate sensorineural hearing loss. He was thus diagnosed to have hereditary arthro-ophthalmopathy and the diagnosis of Stickler syndrome was confirmed.

Stickler syndrome which is also known as hereditary arthro-ophthalmopathy has an autosomal dominant inheritance pattern. (1) The estimated incidence of Stickler Syndrome is 1 in 10,000. (2) It is the most commonly identified inherited cause of retinal detachment in childhood. (3) Mutation in the type II collagen gene locus col2A1 is a causative of Stickler syndrome. It is now known that Stickler syndrome is caused by mutations in four gene loci (col2A1, col11A, col11A2 and col9A1). (4) Though the disorder is not uncommon, it is commonly not diagnosed, due to subtle clinical features. Stickler syndrome should be considered in any neonate with the Robin sequence particularly in those with family history of cleft palate and in patients with dominantly inherited myopia, non traumatic retinal detachment, and/or mild spondyloepiphyseal dysplasia. (1)
The clinical spectrum of Stickler syndrome ranges from severely affected patients to individuals with very mild features. The mildest phenotypes remain undetected, and the disease is, therefore, probably under diagnosed. Because of this phenotypic heterogeneity, clinical diagnosis of Stickler syndrome is difficult. Symptoms become more severe with advancing age. (5) Ophthalmic complications include high degree myopia which develops in 40% of patients before 10 yrs of age and in 75% by age 20 yrs; retinal detachment; cataracts; abnormalities of vitreous formation and gel architecture. (5) Retinal detachment can be prevented by prophylactic laser therapy and cryotherapy. It is to be hoped that detachment can be corrected surgically if recognized early. (6) Musculoskeletal problems include hypotonia, hyperextensible joints, congenital talipes equinovarus (CTEV), subluxation of hip and spondyloepiphyseal dysplasia. Severe arthropathy can occur in childhood with small joint pains simulating juvenile rheumatoid arthritis. Secondary degeneration of articular surfaces occurs in adulthood. (7) Other common anomalies include deafness (both sensorineural and conductive), and mitral valve prolapse. Affected individuals with mitral valve prolapse should be evaluated periodically and should receive infective endocarditis prophylaxis before surgical procedures. (8)
| | | | Keywords | | Stickler syndrome, Pierre Robin anomaly, Spondyloepiphyseal dysplasia | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Jones KL. Smith's recognizable patterns of human malformation. 6th ed. Philadelphia: Elsevier Saunders. 2006; 318-319. [PMC free article]
- Herrmann J, France TD, Spranger JW, Opitz JM, Wiffler C. The Stickler syndrome (hereditary arthroophthalmopathy). Birth Defects Orig Artic Ser. 1975;11: 76-103. [PubMed]
- Carroll C, Papaioannou D, Rees A, Kaltenthaler E. The clinical effectiveness and safety of prophylactic retinal interventions to reduce the risk of retinal detachment and subsequent vision loss in adults and children with Stickler syndrome: a systematic review. Health Technol Assess. 2011; 15: iii-xiv, 1-62. [CrossRef]
- Snead MP, Yates JR. Clinical and molecular genetics of Stickler syndrome. J Med Genet. 1999; 36: 353-359. [PubMed] [PMC free article]
- Stickler GB, Belou PG, Farrell FJ, et al. Hereditary progressive arthroophthalmopathy. Mayo Clin Proc.1965; 40: 433. [PubMed]
- Abeysiri P, Bunce C, da Cruz L. Outcomes of surgery for retinal detachment in patients with Stickler syndrome: a comparison of two sequential 20-year cohorts. Graefes Arch Clin Exp Ophthalmol. 2007; 245: 1633-1638. [CrossRef]
- Hakim H, Elloumi M, Ben Salem M, Karray S, Baklouti S. Polyarthritic manifestations revealing Stickler syndrome. J Radiol. 2002; 83: 1856-1858. [PubMed]
- Admiraal RJ, Szymko YM, Griffith AJ, Brunner HG, Huygen PL. Hearing impairment in Stickler syndrome. Adv Otorhinolaryngol. 2002; 61: 216-223. [CrossRef]
- Saul C, Pias VM, Jannke HA, Braga NH. Endoscopic removal of Ascaris lumbricoides from the common bile duct. Am J Gastroenterol 1984; 79; 725-727. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2012.78
|
| Cite this article as: | | Lakhkar B, Lakhkar B, Abhilasha. STICKLER SYNDROME. Pediatr Oncall J. 2012;9: 113-114. doi: 10.7199/ped.oncall.2012.78 |
|