Rajendra P Karambelkar1, Sachin Shah2, Nisha Deshpande1, Dasmit Singh3.
1Department of Pediatrics, Aditya Birla Memorial Hospital, Chinchwad, Pune, India,
2Department of Neonatology, Aditya Birla Memorial Hospital, Chinchwad, Pune, India,
3Pediatric Surgery, Aditya Birla Memorial Hospital, Chinchwad, Pune, India.
ADDRESS FOR CORRESPONDENCE
Rajendra P Karambelkar, Consultant Pediatrician, Department of Pediatrics & Neonatology, Aditya Birla Memorial Hospital, Aditya Birla Hospital Marg, Chinchwad Pune 411033, India.
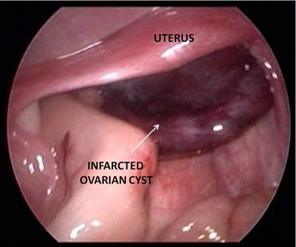
Email: rjkarambelkar@yahoo.co.in | | Keywords | | infantile colic, ovarian cyst, ovarian torsion | | | A 4-month-old female infant presented with bouts of intermittent cry lasting for more than 18 hours without any other complaints. At six hours, they visited the emergency room, where due to lack of any findings parents were reassured and advised further observation at home. However, since crying continued overnight, parents visited the hospital again. She was a full term, exclusively breast-fed and was growing normally. Antenatal ultrasonography in late second trimester had not picked up any fetal abnormality. Feed acceptance, passage of stools and urine was normal. There was a history suggestive of multiple episodes of infantile colic so parents waited in anticipation for relief. Her physical examination was normal except mild tenderness in right inguinal and lumbar area with no palpable mass. An urgent ultrasonography abdomen and pelvis was performed which demonstrated 33mm x 31 mm echogenic lesion in the right adnexal region without any vascularity within. Right ovary was not visualized separately and that lead to a diagnosis of ovarian torsion. On emergency laparoscopy, since right ovary was necrosed along with the torsion of the pedicle (Fig.1) right oophorectomy was performed. Left ovary was normal. Histopathological examination of right ovary showed cystic lesion with extensive calcification and torsion induced changes. Lining epithelium or primordial follicles were absent and there was no evidence of neoplastic process.
Fig.1: Infarcted right ovarian cyst on laparoscopy
Abnormal twisting (axial rotation) of ovary and sometimes-fallopian tube around the ovarian pedicle results in ovarian torsion / adnexal torsion. Incidence of ovarian torsion is estimated to be about 4.9 per 100,000 in females 1-20 years of age (1). It commonly occurs during childbearing age and postmenopausal age (2). Before the onset of menarche, the risk of ovarian torsion is highest in the perinatal period but it is extremely rare in postnatal period and in young children. Ovarian cysts develop in most of the female fetuses (3), however, nearly all the simple cysts resolve spontaneously after birth (4). Presenting symptoms and signs of ovarian torsion are usually nonspecific like lower abdominal pain, fever, nausea and vomiting. Clinical examination may reveal tenderness in lower abdomen and sometimes mass (2). Differential diagnosis includes infantile colic, intussusception, appendicitis, mesenteric lymphadenitis, constipation, acute gastroenteritis, urinary tract infection and ureteric colic. It must be remembered that infantile colic rarely persists beyond 3 months of age (5). Delay in diagnosis of ovarian torsion is common resulting in loss of involved ovary and other complications. Ultrasonography is usually enough for a diagnosis. Emergency laparoscopy must be undertaken for confirmation and treatment of ovarian torsion. Detorsion of ovary with better outcome is possible with early surgical intervention and is recommended. The decision to simultaneously perform an oophoropexy of contralateral ovary is debatable.
Ovarian torsion, though extremely uncommon is not rare in infants. An early diagnosis can salvage the ovary and avoid psychological trauma to the parents and the child. Therefore, high index of suspicion of ovarian torsion must be kept in mind in all the female infants presenting with suspected abdominal pain. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Guthrie BD, Adler MD, Powell EC. Incidence and trends of pediatric ovarian torsion hospitalizations in the United States, 2000-2004. Pediatrics 2010; 125:532-8. [CrossRef]
- Eng-Lunt J, Appelbaum H, Avarello J. Pediatric and Adolescent Ovarian Torsion. ACEP News, December 2011. Available at URL: http://www.acep.org/Content.aspx?id=82860.
- Vogtlander MF, Rijntjes-Jacobs EG, van den Hoonaard TL, Versteegh FG. Neonatal ovarian cysts. Acta Paediatr. 2003; 92: 498-501. [CrossRef]
- Bryant AE, Laufer MR. Fetal ovarian cysts: incidence, diagnosis and management. J Reprod Med 2004; 49: 329-37. [PubMed]
- Heird WC. The Feeding of Infants and Children. In Kliegman, Behrman, Jenson, Stanton editors, Nelson Textbook of Pediatrics, 18 th Edition, 2008. p.222.
DOI: https://doi.org/10.7199/ped.oncall.2013.21
|
| Cite this article as: | | Karambelkar R P, Shah S, Deshpande N, Singh D. OVARIAN TORSION IN A 4-MONTH-OLD BABY. Pediatr Oncall J. 2013;10: 60. doi: 10.7199/ped.oncall.2013.21 |
|