Dr Ira Shah, Kalpana Sengupta.
Department of Pediatrics, B.J. Wadia Hospital for Children, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
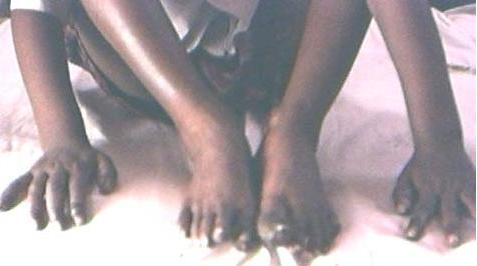
Ira Shah, Department of Pediatrics, B.J. Wadia Hospital for Children, Mumbai 400012. | | Abstract | | Pompholyx is a recurrent, sometimes seasonal vesicular eczema of the hands and feet. Increased sensitivity to metal compounds in addition to local hyperhidrosis has also been postulated as the possible mechanism. We present a case of a pompholyx in a 5 year old child with hyperhidrosis. | | | | Introduction | | Pompholyx is a recurrent, sometimes seasonal vesicular eczema of the hands and feet.(1) Though the pathogenesis is unknown, experts believe that the condition is caused by stress or emotional turmoil.(2) Increased sensitivity to metal compounds in addition to local hyperhidrosis has also been postulated as the possible mechanism.(3) It is also known as Dyshidrosis. Colloidal dressings and topical corticosteroids are used for the treatment with emphasis on avoiding triggering factors such as stress, chemicals and allergens.(1) We present a case of a pompholyx in a 5 year old child with hyperhidrosis. | | | | Case Report | A 5 year old male child presented with small pruritic vesicles over the fingers and toes. These vesicles were present over the volar aspects of the palms & soles and were initially fluid filled. Within 4 days, the vesicles burst & developed secondary infection, maceration and crusting (Fig 1). There was no history of any allergy though the child did complain of increased sweating over the palms soles. There were no previous such episodes. The clinical diagnosis was secondarily infected pompholyx. The child was treated with KMnO4 soaks and topical antibiotics for superadded infection. The lesions improved within 2 days. The child was advised to protect his hands and feet from chemicals & harsh soaps and informed regarding chances of recurrences in future.
Figure 1: Vesicles over palms and toes
 | | | | Discussion | | Pompholyx is a non-inflammatory vesicular eruption in the palms & soles. It is a recurrent disorder with relapses frequently in patients with atopy, hyperhidrosis or neurovegetative states. It presents as severe itching over the hands & feet with appearance of vesicles over the lateral & volar aspect of fingers and toes. These vesicles arise from beneath the stratum corneum in the epidermis and are filled with clear fluid. They become painful as they grow in size.(4) Secondary infection is frequent due to scratching.(1) The vesicles dry up and disappear within 2-3 weeks.(4) With frequent relapses, the skin may become thickened, with uncomfortable fissured plaques. The diagnosis is clinical and may be mistaken for allergic contact dermatitis that usually affects the dorsal surfaces. Treatment consists of wet dressings and topical antibiotics for superadded infection during the acute phase.(1) Topical corticosteroids are the mainstay of treatment in the chronic phase.(5) Other therapies in recalcitrant lesions tried are topical tacrolimus,(5) low dose radiation therapy,(6) azathioprine,(7) low dose oral methotrexate(8) and tap water iontophoresis.(9) Patient education about stress management and use of emollients is vital in preventing recurrence. Patients are also advised to avoid irritant, protect hands and avoid unnecessary exposure.(2) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Behrman RE, Kliegman RM. Nelson Textbook of Pediatrics 15th ed. W.B.Saunders. Bangalore, 2000: 1859. [PMC free article]
- Landow K. Hand Dermatitis, The perennial scourge. Post Grad. Med. 1998; 103: 141-152. [CrossRef]
- okozeki H, Katayama I, Nishioka K, Kinoshita M, Nishiyama S. The role of metal allergy and local hyperhidrosis in the pathogenesis of pompholyx. J Dermatol 1992; 19: 964-967. [CrossRef]
- Lambert D. Dyshidrosis. Rev. Part 1998; 48: 968-970.
- Schnopp C, Remling R, Mohrenschlager M, Weigl L, Ring J, Abeck D. Topical tacrolimus (FK506). and mometasone furoate in the treatment of dyshidrotic palmar eczema: a randomized, observer blinded trial. J Am Acad Dermatol 2002; 46: 73-77. [CrossRef]
- Stambaugh MD, De Nittis AS, Wallner PE, Heymann WR. Complete remission of refractory dyshidrotic eczema with the use of radiation therapy. Cutis 2000; 65: 211-214. [PubMed]
- Scerri L. Azathioprine in dermatological practice. An overview with special emphasis on its use in non-bullous inflammatory dermatoses. Adv Exp Med Biol 1999; 455: 343-348. [CrossRef]
- Egan CA, Rallis TM, Meadows KP, Krueger GG. Low dose oral methotrexate treatment for recalcitrant palmoplantar pompholyx. J Am Acad Dermatol 1999; 40: 612-614. [CrossRef]
- Wollina U, Uhlemann C, Elstermann D, Kober L, Barta U. Therapy of hyperhidrosis with tap water iontophoresis. Positive effect on healing time and lack of recurrence in hand-foot eczema. Hautarzt 1998; 49: 109-113. [CrossRef]
|
| Cite this article as: | | Shah I, Sengupta K. Pompholyx. Pediatr Oncall J. 2009;6: 17. |
|