Dr Sudipta Misra.
Associate Professor of Clinical Pediatrics Chief, Section of Pediatric Gastroenterology, Childrens Hospital of Illinois, USA. | Acute abdominal pain is a common problem in pediatrics. Most of the episodes are benign and resolve with no or minimal intervention. However, a systemic approach is essential in distinguishing children who have serious underlying conditions from those who do not.
How to use this article:
Confronted with acute abdominal pain, the pediatrician should consider if that child
- Have a condition that needs immediate intervention- e.g. intestinal volvulus, intussusception, perforated appendix etc.
- Need immediate investigations to find a cause that may need intervention or prolonged specialized care e.g. acute pancreatitis, appendicitis etc.
- Have a condition that can potentially develop into a serious condition and need to be observed in the hospital e. g sub-acute or intermittent intestinal obstruction, intra-abdominal, hepatic abscess etc.
- Have a benign condition despite severe pain that can be treated at home- e.g. acute gastroenteritis, colic in infants etc.
This article intends to help the physician make that decision based on age of the patient, localization, associated symptoms and insight into some disorders. Table-1 enumerates the common causes of acute abdominal pain at different age groups. Table -2 lists the red flag signs elaborated in the text. The flow charts (Figure -1) are designed to help distinguish between common problems based on localization and symptoms associated with abdominal pain. These have been cross-referenced with signs and symptoms of that particular disorder. The text provides insight into and fallacies of diagnosis of common causes of abdominal pain. It is assumed that the pediatrician has access to basic investigations such as X-ray, ultrasound, blood chemistry and hemogram.
NEWBORN
Abdominal pain in newborns manifests as incessant crying, drawing up of the legs, irritability along with non-specific signs such as poor feeding. Almost every baby has a number of self-limiting episodes of crying supposedly due to abdominal pain. These are to be differentiated from persistent episodes causes by serious conditions (Table -1). Neonatal infection and other non-GI causes can mimic clinical signs of abdominal pain. (See 'Non GI causes of pain in children < 2 years' below).
Rule
The baby is assumed to be having a serious or surgical cause till proven otherwise by examination, investigations and/or observation over time.
Clinical pointers towards possible serious or surgical condition
- Bilious vomiting, constipation, abdominal distension, blood in stool.
- Systemic manifestations such as vascular instability, lethargy, shock. Hypo or hyperthermia.
- Tense, tender, discolored abdomen, absent or hyperactive bowel sounds on examination.
- Irreducible bulge in the inguinal area suggestive of incarcerated inguinal hernia.
Initial investigation of choice
Plain x-ray abdomen is the initial investigation of choice. Though widely available, this investigation is often improperly done. The technician should adjust the exposure to size of the baby so that the abdominal gas pattern, fluids and abdominal viscera are properly visualized. Exposure suitable for adults or chest x-rays may be unsuitable for this purpose. To distinguish air fluid level and free air under the diaphragm, the baby should be held in an upright posture during and 5 minutes prior to the exposure. If this is not possible, a cross-prone lateral film may be attempted. A shorter exposure time may be required to decrease movement artifacts in an un-cooperative infant. The plate should include lower part of chest with both domes of the diaphragm and the whole abdomen including the rectum. The x-ray should be reviewed by a physician familiar with signs such as pneumatosis intestinalis, portal vein gas, abnormal gas distribution in the bowel, fixed, localized dilatation of the bowel loops etc.
Referral
The threshold for referral for specialized care should be low in newborns. If the crying episodes and abdominal pain are persistent, significant and an obvious cause such as constipation with stool impaction cannot be found, investigations and referral should be considered.
CHILDREN BELOW 2 YEARS OF AGE
At this age, abdominal pain is manifest by poor localization with non-specific signs such as crying, irritability etc. At times, it may not be obvious that the abdominal pain is the cause of the problem.
The chief concerns in this age group are
- Acute intermittent recurrent episodes of abdominal pain Acute intermittent recurrent episodes of abdominal pain
- IntussusceptionIntussusception
- Toxin ingestion Toxin ingestion
- Trauma, accidental or due to child abuse Trauma, accidental or due to child abuse
- Non GI causes of pain Non GI causes of pain
Acute intermittent abdominal pain: This is the most common form of pain in children below 6 months. This may have to be differentiated from the pain of intussusception. Common causes include
Infantile colic: It is defined as at least 3 hours of inconsolable crying occurring at least 3 times a week for 3 weeks with clustering of the episodes in the evening. It usually starts early and resolves around 4-5 months of age. There may be a positive family history in siblings or parents. Though the typical picture is characteristic, atypical cases may need to be differentiated from other causes especially gastroesophageal reflux. Most of the treatment modalities are of doubtful clinical use. Tactile stimulations such as skin-to-skin contact and gentle rocking at the very onset of an episode, often associated with a change in arousal level, may abort an episode.
Gastroesophageal reflux: The esophageal symptoms of gastroesophageal reflux may cause significant irritability, crying and abdominal pain. These symptoms are likely to be caused by acid injury to the esophageal mucosa. Symptoms due to non-acid reflux (non erosive esophagitis) is a possibility but has not been documented in infants. Typically, these children present with vomiting, irritability, arching back, feeding difficulty or refusal and interrupted sleep. Associated features may include growth failure or respiratory symptoms. Esophageal symptoms are among the 'red flag signs' for gastroesophageal reflux. It should be treated with acid suppression and anti reflux measures. If complete resolution of symptoms is not achieved, referral for specialized care should be made.
Infantile dyschezia: This typically occurs in infants in their first month of life. This children strain, cry and show other signs of distress for more than 10 minutes before defecation. Ultimately the child passes a soft stool followed by resolution of symptoms. These recurring symptoms may be stressful to the parents and mimic other serious causes of abdominal pain. The typical history is the lynch pin of diagnosis of this condition. Basically, the infant is learning to coordinate the relaxation and contraction sequences of various muscles required for successful defecation. Unsuccessful attempts of defecation are the cause of symptoms in these infants. Most important component of management of this condition is reassuring the parents, emphasizing the pathophysiology and benign nature of the condition. As the child get his act together, the symptoms gradually improve within weeks to months. No active intervention is required. Measures like perianal stimulation may actually perpetuate the dyschezia.
Intussusception: Typically, a completely normal and healthy child between the ages of 2 months and 5 years presents with history with intermittent acute abdominal pain with pain free intervening period. The clinician should be sensitive to the possibility of intussusception in all infants in this age range with acute intermittent abdominal pain. Textbook clinical signs such as blood in stool appear late and by that time the intussusception may be irreducible and/or bowel necrosis might have set in. Clinical signs such as 'sausage' in the abdomen has been reported to be present in as much as 65% of these infants. However, in our experience, it is not a reliable clinical marker. Plain X-ray abdomen and ultrasonography are diagnostic while barium or air contrast enemas are diagnostic as well as therapeutic.
Toxin ingestion: Children acquire mobility at this age and are in oral phase of development. These children are vulnerable to accidental toxin or foreign body ingestion. The characteristic history is sudden onset of symptoms, vomiting, irritability and/or abdominal pain. Oral lesions, drooling of saliva and respiratory symptoms such as stridor or wheezing can be present with corrosives. Iron pill ingestion can cause vomiting and abdominal pain followed by hepatic failure. Vomiting and abdominal pain are the initial symptoms of suicidal attempts by acetaminophen ingestion in adolescents. A chronological history of the events leading up to the symptoms is essential. Every attempt should be made to identify the ingested agent.
Trauma: Child abuse is an important cause of abdominal pain at this age. The relationship between abdominal pain and trauma is elaborated below under 'Children above 2 years of age'.
Non-Gastrointestinal (GI) causes of pain: Infants tend to stiffen up, arch back or even draw their legs up in response to any significant pain. Due to non-specific and poorly localized nature of nociceptive response, pain caused by non-GI lesions may be mistaken for abdominal pain. Corneal foreign bodies are an important example of such pain. At times, eye examination after fluorescein instillation may be required to detect corneal abrasion. Fracture (due to child abuse), forgotten tourniquet, foreign bodies such as needles or nails lodged in the soft tissues and osteomyelitis are some other common examples non GI lesions masquerading as abdominal pain. A through examination of the infant is warranted if no apparent cause for his irritability and crying can be found.
CHILDREN ABOVE 2 YEARS OF AGE
These children, especially the older ones can verbalize their symptoms, which help a lot with localization. It is important to separate the serious causes from the relatively benign ones. The so-called red flag signs that should prompt immediate investigations include
Bilious vomiting: As a general rule, in medical conditions such as gastroenteritis, vomiting precedes or accompanies abdominal pain. In surgical conditions such as intestinal obstruction and appendicitis, pain precedes vomiting. However, in upper gastrointestinal obstruction, vomiting may occur early. Though bile can appear in vomitus with prolonged vomiting, bilious vomiting with abdominal pain is an ominous sign. Gastrointestinal obstruction, especially of the proximal bowel, should be ruled out. Contrary to popular belief, malrotation with volvulus can present at even in mature adulthood. Immediate intervention can save the intestine from being necrosed. Plain X ray abdomen and carefully done water soluble contrast study of the upper GI tract can detect obstruction. If gastrointestinal obstruction is ruled out, then medical conditions such as acute cholecystitis and pancreatitis should be considered.
Peritonitis: Shining tender abdomen with rebound tenderness is characteristic of peritonitis. However, these are late signs and their presence usually mean significant peritoneal contamination leading to increased morbidity and mortality. All attempts should be made to diagnose peritonitis early. Being vigilant about the possibility of peritonitis in vulnerable population can lead to early diagnosis. For example, children with suspected appendicitis, intestinal perforation (obstruction, trauma), ascitis, on chronic peritoneal dialysis, ventriculo-peritoneal shunt, asplenia or splenectomy, immunodeficiency etc. should be watched carefully for early signs of peritonitis.
The diagnosis of peritonitis in primary care facilities is mostly clinical with investigations for intestinal perforation (free gas in the peritoneum) and features of generalized infection such as raised white blood cell count with a left shift. CT scan and peritoneal tap can confirm the diagnosis in a specialized center.
Abdominal distension with or without visible peristalsis and altered bowel sound: This is the textbook picture of intestinal obstruction and needs surgical care. However, in less obvious cases, acute gastroenteritis can mimic intestinal obstruction with mild abdominal distension, vomiting, increased bowel sound (cf. early phase of mechanical obstruction), ileus due to dyselectrolytemia and air fluid levels (usually less numerous than in obstruction) on X-ray abdomen. Careful observation over time helps to differentiate between these two. The child with acute gastroenteritis with the above-mentioned signs requires inpatient care including intravenous fluid and electrolytes.
History of intra-abdominal surgery: Any child with history of abdominal surgery and abdominal pain with or without vomiting should be presumed to be having complications from surgery till proven otherwise. In the first 6 weeks post surgery, common complications include local site infection, intra abdominal abscess due to leakage from the anastomosis, intra-abdominal hematomas, peritonitis and intestinal obstruction. After 6 weeks, partial, intermittent or complete intestinal obstruction may occur due to fibrous band formation.
Plain X-Ray abdomen is an excellent screening investigation. Ultrasound and or CT scan may be required for defining intra abdominal lesions.
Blood in stool with abdominal distention and tenderness: Though any dysentery can present with these features, one should be aware of the possibility of a developing megacolon. Both infectious and idiopathic inflammatory bowel disease can cause megacolon. Usually these children show systemic signs such as vasomotor instability, fever, lethargy etc. Serial abdominal girth measurement and abdominal X-rays are useful in diagnosing this condition.
Immediate decompression with a rectal tube is warranted followed by referral for specialized care.
Hematemesis and abdominal painHematemesis and abdominal pain: This is characteristic of erosive gastritis or acid peptic disease. History of non-steroidal anti-inflammatory drugs (NSAID) intake is an important pointer towards this condition. Any NSAID, even COX-2 inhibitors, can cause gastric mucosal injury. Past history of heartburn, epigastric pain and family history are important pointers towards acid peptic disease with bleeding. However, if blood appears in later episodes of vomiting, secondary causes of bleeding such as Mallory-Weiss tear(s) and traumatic gastropathy should be considered. Bleeding from esophageal varices may be associated with a less severe abdominal pain.
Hemodynamic stabilization with crystalloid, colloid and packed RBC infusion is of paramount importance at the primary care setting. Empirical intravenous acid suppression therapy, preferably with a proton pump inhibitor, should also be initiated.
Children who do not have the red flag signs may still have potentially serious disease but can be treated or watched in good medical facility. Common cause of such abdominal pain include:
Acute gastroenteritis: It's a common, easily manageable cause of abdominal pain in all ages. However, at times it may mimic more serious conditions. Vomiting preceding or occurring along with abdominal pain, non-bloody diarrhea and history of contact with persons with similar symptoms with or without fever are the cornerstones of this diagnosis. It may be associated with mesenteric lymphadenitis (see below).
Appendicitis: This condition should be considered in any right lower quadrant abdominal pain. However, definitive diagnosis depends on evolution of the disease process under close clinical monitoring, white blood cell count, ultrasound and CT examination of the abdomen. Appendicitis, though rare in non-verbal young infants, can be dangerous. Its initial presentation may be peritonitis due to perforation. In older children, sudden relief of pain may indicate perforation and impending peritonitis.
Constipation: Constipation with stool impaction can present with severe abdominal pain, abdominal distention and even vomiting at all ages. It is a relatively common cause of abdominal pain in children of all ages. A simple per rectal examination can be diagnostic. History of constipation, soiling and palpable sigmoid colon also help in the diagnosis. Signs of constipation should be looked for in all abdominal X-rays taken for acute abdominal pain.
Trauma: Abdominal trauma due to child abuse or accident can present with acute onset abdominal pain and/or irritability. The pain may be due to rupture or hematoma of a hollow viscus, most commonly the second and third parts of the duodenum. These areas are vulnerable as they are fixed retroperitoneal structures overlying the vertebral column. Duodenal hematomas present with features of upper intestinal obstruction, bilious vomiting without abdominal distension usually 2-3 weeks after injury. Intestinal perforation may manifest as peritonitis. Rupture or laceration of solid viscus such as spleen and liver can cause significant bleeding leading to shock. Blunt trauma of the abdomen is the commonest known cause of pancreatitis in children. Carefully taken history should be correlated with the external marks and nature of injury. Free air by plain X-ray abdomen may indicate hollow viscus perforation or rupture. Referral for CT scan abdomen should be considered to detect solid organ laceration, hematomas and intraperitoneal bleeding.
Functional abdominal pain and other motility disorders: These children may present with severe acute abdominal pain. Past history of chronic abdominal pain, paucity of signs compared to the symptoms of the child and negative screening tests should alert the clinician to this possibility. Unnecessary laparotomy, cholecystectomy and other surgical procedures have been performed on these children due to lack of familiarity with this condition. However, a child with functional disorder can develop acute conditions such as appendicitis, which may need surgical intervention.
Acute pancreatitis: Children with unexplained acute abdominal pain should have serum lipase and amylase measured to exclude pancreatitis. Though abdominal pain, vomiting and nausea are characteristic, many lack the classical features. Studies in adults show that though most of the amylase and lipase estimations are normal, many cases of subtle pancreatitis would have been missed if these tests were not routinely ordered. The etiology of 80% of pancreatitis in children is unknown. The commonest known cause is blunt abdominal trauma followed by anatomical abnormalities such as pancreatic divisum and cholelithiasis in children with hemolytic anemia. Some children may have recurrent episodes while others show a familial tendency.
Acute Cholecystitis: Upper abdominal pain with nausea and vomiting are characteristics for acute cholecystitis. It can be due to cholelithiasis or it can be acalculous cholecystitis (hydrops of the gall bladder). Abdominal ultrasound is helpful in making this diagnosis. Failure to visualize the gall bladder by HIDA scan confirms the diagnosis.
Pneumonia: Pain from lower lobe pneumonia with pleuritis can be referred to the same dermatomes- T 9 and 10, on the abdomen. These dermatomes supply the epigastric and umbilical areas. Signs of respiratory infection including fever and dyspnea, distribution along characteristic dermatomes and lack of abdominal signs should alert the physician to this possibility. Chest X-ray is diagnostic. Some recent evidences suggest that associated mesenteric lymphadenitis may be responsible for abdominal pain in children with pneumonia.
Mesenteric lymphadenitis: Fever, vomiting and upper respiratory tract infection accompanied by crampy abdominal pain is the typical clinical presentation of this self-limiting mostly viral syndrome. There is no abdominal tenderness, abnormal bowel sounds or palpable mass. It may resemble surgical abdomen. Ultrasound or CT scan, which shows enlarged lymph nodes in the mesentery, mostly near the terminal part of the ileum, is useful in making a diagnosis.
Abdominal Migraine: These children have recurrent episodes of acute abdominal pain lasting for hours to days. Recurrent nature of the pain episodes, history of prodromes, family history of migraine and negative abdominal examinations and screening tests points towards this diagnosis. Paradoxically, headache is rare in these children.
Henoch Schnolein Purpura: This condition can cause acute abdominal pain and gastrointestinal bleeding. Abdominal pain can precede characteristic raised lower extremity rashes. In some cases the rashes may never appear. This is a clinical diagnosis of exclusion.
Investigations at the primary care setting:
Plain X-Ray abdomen: This simple, almost universally available investigation is an excellent tool in investigating the cause of acute abdominal pain. For fallacies of this test see above under "newborns".
Abdominal Ultrasound: Popularity of this test stems from its wide availability, being non invasive and inexpensive. However, ultrasound is highly operator dependent, especially for subtle signs such as those for appendicitis, intussusception, etc. An experienced ultrasonologist should be utilized for maximum benefit.
Blood tests: Serum lipase and amylase estimation is useful in evaluating acute abdominal pain in children. Other blood test such as complete blood count and metabolic profile are useful as circumstantial evidence for the cause of abdominal pain.
Other tests: CT scan, MRI scan, Endoscopy, ERCP etc are more suitable for secondary and tertiary care settings.
Table -1.Common Causes of Abdominal Pain
| Newborn | Infants < 2 years | Intestinal Obstruction- Intestinal atresias and stenosis
- Meconium Ileus and/or irschsprung's diseases
- Malrotation and volvulus
- Post intra abdominal surgery
Peritonitis- Spontaneous perforation of the stomach or intestine
- Due to intestinal obstruction
- Neonatal necrotizing enterocolitis
Others- Incarcerated hernia with bowel necrosis or ovarian torsion
- Gastroesophageal reflux
- Abdominal trauma (difficult birth)
| - Colic
- Infantile dyschezia
- Gastroesophageal reflux
- Non-Gastrointestinal causes
- Intussusception
- Malrotation and volvulus
- Incarcerated hernia with bowel necrosis or ovarian torsion
- Acute gastroenteritis
- Abdominal trauma
- Constipation
- Toxin ingestion
| Children (2-18 years) | Adolescents (12-18 years) | - Acute gastroenteritis
- Urinary tract infection
- Constipation
- Streptococcal pharyngitis
- Food poisoning
- Mesenteric lymphadenitis
- Appendicitis
- Intestinal obstruction
- Pneumonia
- Abdominal trauma
- Testicular torsion
- Pancreatitis
- Henoch-Schnolein purpura
- Acute cholecystitis
- Abdominal migraine
| - Suicidal toxin ingestion (acetaminophen)
- Dysmenorrhea
- Mittleschmerz
- Pelvic Inflammatory Disease
- Threatened abortion
- Ectopic pregnancy
|
Table -2. "Red Flag Signs" for Acute Abdominal Pain in Children
- Signs Bilious vomiting
- Signs History of intra abdominal surgery
- Signs Features of peritonitis
- Signs Blood in stool
- SignsBlood in vomitus
- Signs Features of Intestinal obstruction
- Signs Abdominal distension
- Signs Systemic signs
Figure 1
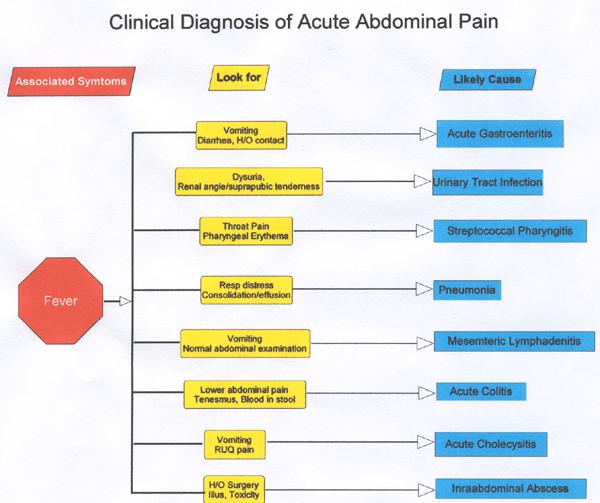
Figure 2
Figure 3
 | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
| Cite this article as: | | Misra S. APPROACH TO ACUTE ABDOMINAL PAIN IN CHILDREN. Pediatr Oncall J. 2005;2. |
|