Dr Vishal Dublish1, Dr Ira Shah2.
1Medical Sciences Department, Pediatric Oncall, Mumbai,
2Incharge,Pediatric Tuberculosis, HIV and Liver Clinic, B.J.Wadia Hospital for Children, Mumbai. | ARDS is a clinical syndrome first described by military physicians during World War I & II. Initially "A" stood for "adult" to differentiate it from infantile RDS. But now "A" stands for "acute". ARDS is characterized by:
Increased permeability of alveolar capillary membrane.
Diffuse alveolar damage.
Accumulation of proteinaceous pulmonary edema.
Originally most definitions of ARDS required three general criteria:
Severe hypoxemia
Reduced pulmonary compliance and
Diffuse pulmonary infiltrates on chest X-RAY
Recently American - European consensus conference proposed a new definition of ARDS, which is new uniformly accepted.
| | Timing | Oxygenation | X-ray chest | Pulmonary artery Occlusion pressure | | Acute lung Injury (ALI) | Acute Onset | PaO2 / FiO2 < 300 mm Hg (regardless of PEEP) | Bilateral Infiltrate | < 18 mm Hg or No evidence of left AtrialHypertension | | ARDS | Acute Onset | PaO2 / FiO2 < 200 mm Hg (regardless of PEEP) | Bilateral Infiltrate | < 18 mm Hg or No evidence of left Atrial Hypertension |
Predisposing factors:
Direct injury to alveolar epithelium
Aspiration of gastric contents
Diffuse pulmonary infection
Toxic inhalation
Near drowning etc
Indirect lung injury via hematogenous delivery of inflammatory mediators
Severe sepsis
Trauma (non-thoracic)
Hypertransfusion
Pancreatitis
Falciparum malaria
Cardiopulmonary bypass, etc.
Clinical features:
ARDS usually occurs within 4-5 days of the initial at-risk diagnosis in majority of patients. In more than 50% of patients, ARDS develops in the first 24 hours. Earliest clinical sign is tachypnea followed by dyspnea.
Lab investigations:
There are no characteristic abnormalities in ARDS, except related to a specific underlying condition e.g. leucocytosis in sepsis, raised serum amylase in pancreatitis, etc.
Chest X-Ray: Initially may be normal but soon diffuse bilateral interstitial or alveolar infiltrates develop.
CT scan (Chest): Heterogeneous pattern with a predominance of infiltrates in the dependent regions of lungs.
Pathophysiology:
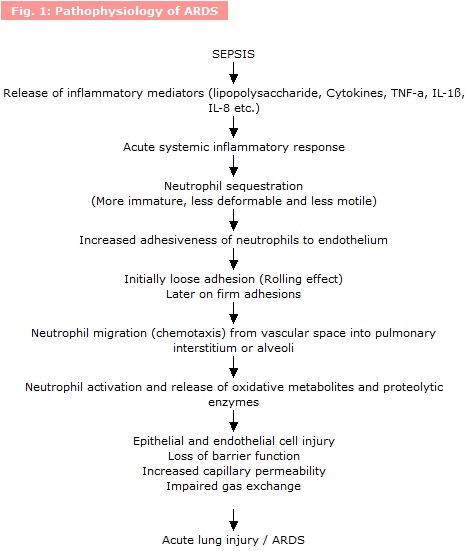
ARDS may be the pulmonary manifestations of a systemic process and is the consequence of an over expression of the normal inflammatory response. There are 3 overlapping phases in inflammatory cascade (Fig. 1):
- Initiation: Any precipitating event (e.g. sepsis) causes production of variety of mediators and cytokines (TNF - a, IL-1) by immune or non-immune cells.
- Amplification: Effector cells e.g. neutrophils are activated recruited and retained in specific target organs such as lungs. Interleukin - 8 (IL-8) is important for activation and released by monocytes.
- Injury: Production of reactive oxygen metabolites and proteases causing cellular damage.
Pathophysiologic hallmark of ARDS is increased vascular permeability to proteins. Even mild increase in pulmonary capillary pressure (because of increased intravascular fluid or myocardial depression) causes increased interstitial and pulmonary edema.
Alveolar damage occurs also because of:
Quantitative reduction of surfactant synthesis due to injury to type-II pneumocytes
Qualitative abnormality in size, composition and metabolism of the remaining surfactant pool causing alveolar collapse.
There is increased pulmonary airway resistance due to:
Bronchial wall edema
Cytokine-mediated bronchospasm
Effect on pulmonary vasculature: Pulmonary artery pressure and pulmonary vascular resistance may be increased due to following reasons:
Increased pulmonary vascular smooth muscle tone
Perivascular edema
Microvascular thrombosis
Humoral factors e.g. - leukotrienes, thromboxane-A2 causing vasoconstriction
Pathology of ARDS - 3 distinct phases:
- Exudative phase: Starts within few days after lung injury. It is characterized by:
Extensive epithelial cell injury especially to type I pneumocytes and basement membrane denudation.
Swelling of endothelial cells with widening of intercellular junctions.
Formation of hyaline membrane composed of fibrin and other matrix protein in alveolar ducts and airspaces.
Neutrophilic infiltration
Fibrin thrombi in alveolar capillaries and small pulmonary arteries.
- Proliferative phase: This phase is most prominent in second or third week after onset of symptoms and is characterized by:
Resolution of neutrophilic infiltration
Cuboidal type II cells and squamous epithelium cover over denuded alveolar basement membrane
Migration of fibroblast and myofibroblasts through breaks in alveolar membrane
- Fibrotic Phase: After few weeks. It is characterized by :
Architectural resolution of lung tissue
Type III elastic collagen is replaced by Type I rigid collagen causing stiff lung.
Interstitial fibrosis with or without cystic and honeycomb changes leading to chronic pulmonary dysfunction and/or death.
Statistical Facts of ARDS and sepsis:
Sepsis especially gram negative with shock is the most common and frequent risk factor.
Frequency of ARDS with sepsis is 18-38%.
18-25% of patients with gram negative sepsis develop ARDS.
Bacteremia with sustained hypotension is the harbinger for development of ARDS.
30% of patients with septic shock develop ARDS while only 14% of patients with sepsis without shock develop ARDS.
When dic is present, 38% patients developed ARDS, while only 17% developed ARDS when dic was not present.
Management:
Once ARDS sets in, it is a challenging task to manage. Still supportive therapy remains the first line of treatment.
General supportive management:
- Treatment of Sepsis: Sepsis should be aggressively treated with an adequate antibiotic regimen. Nosocomial infections should be prevented.
- Fluid management: It is suggested that reduced pulmonary artery pressure, weight loss and fluid restriction may improve outcome in ARDS including time on mechanical ventilation and days in intensive case unit. Increased intravascular hydrostatic pressure causes more alveolar fluid leakage and oxygenation worsens. Fluid restriction or diuretic may worsen shock by reducing cardiac output and organ perfusion. Optimal fluid management for patients with ARDS requires a balancing act between fluid restriction and fluid administration. Recent recommendations are in favor of small reduction in intravascular volume with diuretic use causing significant reduction in the extravascular lung water.
- Mechanical ventilation: is the mainstay of treatment. Goals of ventilatory support include:
Improving gas exchange
Reduce work of breathing
Avoiding oxygen toxicity
Minimizing high airway pressures
Promoting alveolar recruitment
Avoiding further lung damage and
Permitting lung tissue healing
This approach is called as "LUNG PROTECTIVE AND PRESSURE LIMITED STRATEGY"
Recent recommendations are:
- Using small tidal volumes (5-8 ml/kg).
- Longer inspiratory time via volume cycled ventilation or pressure targeted ventilation not to exceed transpulmonary pressure
30-35 cm of water.
- Upward titration of PEEP (Peak end expiratory pressure).
- Allowing permissive hypercapnia, if necessary to reduce transpulmonary pressures.
- Prone position ventilation: May improve oxygenation in more than 75% of ARDS patients. Proposed mechanisms are:
Redistribution of ventilation in the dependent lung zones with improved alveolar recruitment.
Increased drainage of airway and pharyngeal secretions
Redistribution of perfusion to less injured lung regions
Increased functional residual capacity (FRC)
Change in regional diaphragm motion
- Limitations - Chances of extubation, central venous catheter removal, etc.
- High frequency ventilation : It offers an opportunity to use small tidal volumes to prevent ventilation associated lung injury from over distention, and allows higher PEEP with increased recruitment of alveoli. Nearly normal PCO2 can be maintained with high frequency ventilation.
- Partial liquid ventilation : Perfluorocarbon is radio-opaque, inert and colorless liquid that carries a large quantity of oxygen and carbon dioxide. It reduces surface tension and maintains patency of surfactant deficient alveoli. It redirects blood flow to improve ventilation - perfusion ratio. Patient can be safely and adequately oxygenated and ventilated with routine mechanical ventilation.
- Inverse ratio ventilation :
When inspiratory time is kept more than expiratory time (more than half of respiratory cycle) I:E > 1:1. It maintains higher mean airway pressure (MAP) which is a major determinant of oxygenation with lower peak inspiratory pressures (PIP).
Disadvantage: Dynamic hyperinflation may occur because of low expiratory time.
Other Supportive Therapies
- Inhaled nitric oxide (INO): In ARDS, pulmonary vasoconstriction causes increase in pulmonary arterial pressure which may lead to right ventricular dysfunction. Right ventricular ejection fraction (RVEF) is reduced with reduced cardiac output.
Mechanism of action:
It reduces regional pulmonary vascular resistance of ventilated areas.
Helps in reducing intrapulmonary shunting.
Selectively reduces pulmonary artery pressure without systemic vasodilation and hypotension. As off now it is unknown whether iNO reduces mortality rates in ARDS patients.
- Surfactant replacement: Surfactant therapy appears to be an attractive treatment modality in view of quantitative and qualitative abnormalities in surfactant in ARDS patients. Currently studies are on regarding different surfactant preparations, dose and modes of administration.
- Pharmacological Therapy Corticosteroids: Steroids may be helpful in view of their potent anti-inflammatory effects, but not beneficial in early course of disease. Steroids may be of benefit when given after 7 days of unresolving ARDS (fibroproliferative phase). Before starting steroids, systemic infection should be treated adequately or ruled out.
- Ketoconazole: It is an anti fungal agent and is a potent inhibitor of thromboxane A2 which is an important mediator in septic shock and development of ARDS. Few preliminary studies have shown encouraging results in preventing ARDS in patients who are at risk (e.g. sepsis).
- Immunonutrition: It is observed that
Low carbohydrate and high fatty diet reduces ventilatory demand in patients with respiratory failure.
Recent studies suggest that this diet when supplemented with Cicosa-pentanoic acid (CPA), - linoleic acid and antioxidants-
Reduces pulmonary neutrophil recruitment
Improves gas exchange
Reduce duration of ventilation and
Decrease risk of development of new organ failures
- Weaning from ventilator: Weaning can be done when all of the following criteria are met:
- FiO2 < 0.40 and PEEP < 8 cm of water
- Patient is not on neuromuscular blocking agent.
- Inspiratory efforts are apparent.
- Systolic blood pressure > 90 mm Hg without vasopressor support.
Prognosis / Outcome :
Cause of death in ARDS:
Early (within 72 hours) - attributed to the original presenting illness or injury.
Late (after 3 days) - Because of secondary infections, sepsis, persistent respiratory failure and Multi organ dysfunction syndrome (MODS).
In survivors pulmonary functions improve by 3 months and reach maximum levels of correction by 6 months after extubation. 50% of these patients have abnormal lung functions studies such as restrictive impairment or reduced diffusing capacity. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
| Cite this article as: | | Dublish V, Shah I. ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS). Pediatr Oncall J. 2005;2: 48. |
|