Saba Momin, Sabir Patel.
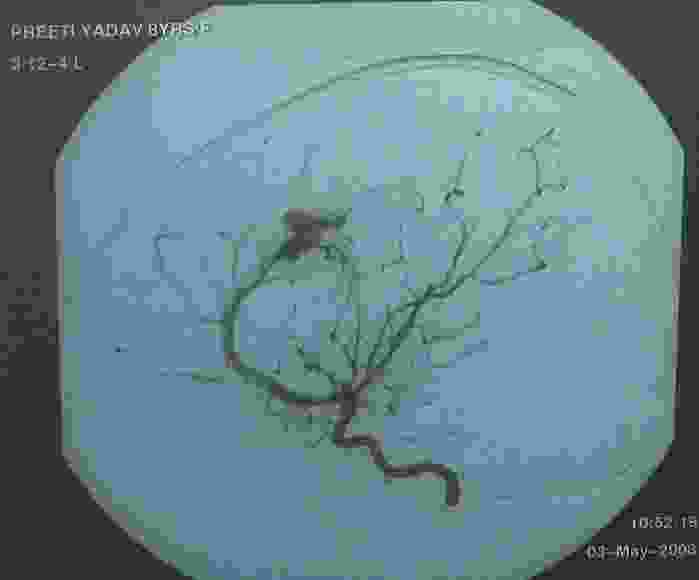
Department of Pediatrics, Dr. R N Cooper hospital, Mumbai, India. | An 8-year-old girl was brought with history of sudden onset headache , loss of consciousness with right-sided hemiparesis . There was one episode of focal convulsion in the form of twitching of the facial muscles. There was no history of trauma or antecedent surgery, cyanotic heart disease, dehydration, tuberculosis (TB) or bleeding manifestations. On examination child was unconscious, responding only to deep painful stimulus. She had spasticity and weakness in right upper and lower limb, planter reflex was extensor in right lower limb . There were no involuntary movements, cerebellar signs or meningeal signs. Other systemic examination was normal. Baseline investigation like complete blood count, x ray chest, urine routine, coagulation profile and screening for TB were noncontributory. CT brain showed large intracranial hematoma with bleed 5 x2.2 cm in the left fronto parietal region with midline shift of 6 mm to the right. Digital subtraction angiography (DSA) shows diffuse slow flow moderate size arteriovenous malformation in left parietal region. (Figure 1)
Figure 1: Arteriovenous malformation in left parietal region on digital subtraction angiography.
In majority of cases, hemorrhagic strokes will reveal themselves with an altered level of consciousness but might also be less symptomatic with headaches, vomiting, seizures and focal neurological deficits. The average incidence of hemorrhagic stroke in children is reported to be between 0.74 - 1.1 / 100000 / year.(1-3) Commonest cause of spontaneous intracerebral hemorrhage in children is arteriovenous malformations (47-55%) .(4) Arteriovenous malformation (AVM) are characterized by presence of arteriovenous shunts through a nidus of abnormal thin walled, coiled tortuous connections between feeding arteries and draining vein , without an intervening capillary network. The vascular channels are separated by glial tissues. The annual risk of hemorrhage in children with known AVM is 2-4 %, in around 25 % cases the hemorrhage is fatal.(4)Although digital subtraction angiography (DSA) is considered gold standard, CT scan with contrast is very often a valuable tool in the precise delineation of the site and cause of hemorrhage in most cases. Management of cerebral vascular malformation , necessitates a multidisciplinary approach involving a vascular neurosurgeon , an interventional neuroradiologist and a pediatric neurologist . Multimodal treatment options are frequent and have to be planned from the beginning. An AVM may be treated by microsurgery, by endovascular approach and with radiosurgery. The presence of life threatening mass effect necessitates immediate surgical treatment.(5) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Eeg-Olofsson O, Ringheim Y. Stroke in children. Clinical characteristics and prognosis. Acta Paediatr Scand. 2001 83;72(3):31.
- Jordan LC, Hillis AE. Hemorrhagic stroke in children. Pediatric Neurol. 2007;36(2):73-80. [CrossRef]
- Celli P, et al. Cerebral arteriovenous malformations in children. Clinical features and outcome of treatment in children and in adults. Surg Neurol. 2001 84;22(1):43.
- Al-Jarallah A, et al. Nontraumatic brain hemorrhage in children: etiology and presentation. J Child Neurol. 2000;1: 284. [CrossRef]
- Humphreys RP, Hoffman HJ, Drake JM, Rutka JT. Choices in the 1990s for the management of pediatric cerebral arteriovenous malformations. Pediatric Neurosurg 1996;25:277-285. [CrossRef]
|
| Cite this article as: | | Momin S, Patel S. Hemorrhagic Stroke in a Case of Arteriovenous Malformation. Pediatr Oncall J. 2009;6: 29-30. |
|