A K Singh, Prakash K Khetan, Chhitij Srivastava, Sanjeev Dua, Vikas Gupta, Sushma Dokania, Y P Bundela, Vimal Agarwal.
Department of Neurosurgery, Fortis Hospital, Noida, India.
ADDRESS FOR CORRESPONDENCE
Prakash K Khetan, Department of Neurosurgery, Fortis Hospital, B-22, Sector-62, Noida, India.
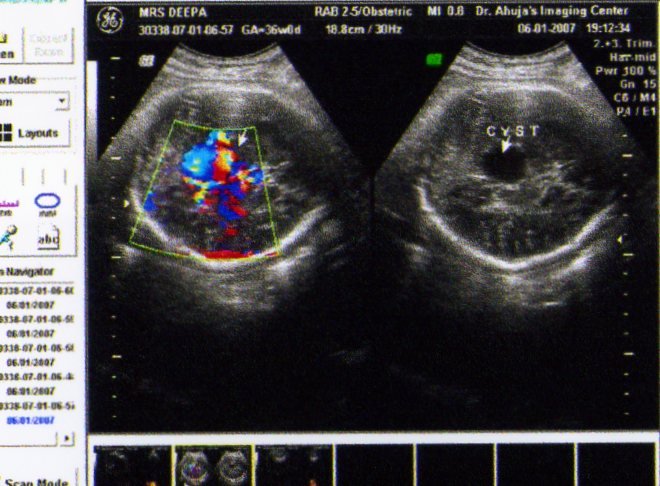
Email: khetanprakash@yahoo.co.in | | Abstract | | Vein of Galen Aneurysm (VOGA) is a rare congenital malformation of brain. Most cases present in neonatal life with congestive cardiac failure. We report a case of Aneurysm of vein of Galen diagnosed in intrauterine life at 36 weeks of gestation who was delivered normally with normal cardiac parameters. The importance of third trimester ultrasound with Doppler evaluation and post-natal confirmation of diagnosis is highlighted. | | | | Introduction | | Vein of Galen Aneurysm (VOGA) are rare anomalies of intracranial circulation that constitute 1% of all intracranial vascular malformations (1). These lesions are characterized by the presence of dilated midline deep venous structure, fed by abnormal arteriovenous communications. VOGA are believed to result from an insult to the cerebral vasculature between 6 and 11 weeks of gestation (2). Prenatal diagnosis is usually possible in the third trimester of pregnancy (3), but still most cases are diagnosed postnatally (4). | | | | Case Report | A 22 years old woman reported for routine ultrasound evaluation at 36 weeks of pregnancy. Her previous two ultrasounds at 14 and 27 weeks of gestation were normal. Ultrasound examination done at 36 weeks revealed a well-defined anechoic cystic lesion of about 2.2 x 2.0 cm size present intracranially in midline at the level of mid brain and was extending posteriorly below the splenium. There was no calcification and hydrocephalus (Figure 1). Doppler ultrasound of brain revealed a cystic area in mid line at the level of mid brain with turbulent flow in it (Figure 1). Fetal heart showed normal right ventricle and normal pulmonary artery with no evidence of hyperdynamic circulation. On the basis of ultrasound findings a diagnosis of vein of Galen aneurysm was made and parents were counseled for the outcome. A baby boy was born by normal spontaneous delivery. His weight was 3.2 kg. Postnatally CT scan and MRI brain was done to detect the lesion which was confirmed by Digital Subtraction Angiography. Chest radiographs does not reveal any features of congestive heart failure. Baby was closely monitored at home and at the age of 3 months, weight of baby was 5.4 kg and on imaging features of cerebral parenchymal damage in the form of diffuse chronic ischemic changes was absent with no evidence of hydrocephalus or high output cardiac failure.
Figure-1. Contrast CT showing subdural empyema over left cerebellar hemisphere with mid-ipsilateral cerebellar oedema
 | | | | Discussion | Vein of Galen is a short midline venous structure formed by the confluence of the two internal cerebral veins and the basal veins of Rosenthal. It represents the caudal remnant of the median prosencephalic vein, a centrally located vessel that drains the choroid plexus. Yasargil classified VOGMs into four categories (5).
Only few cases of VOGA are diagnosed in utero. About 40% of cases are diagnosed in the neonatal period (4) while the rest are diagnosed later in life. Antenatal diagnosis is usually made after the 30th week of gestation because the malformation grows as pregnancy advances. Therefore, the importance of third trimester ultrasound is emphasized (3). The widespread use of routine antenatal ultrasonographic examinations has enabled the detection of several cases of VOGA in the third trimester of pregnancy (6-9). Apart from identification of the abnormality and its differentiation from other nonvascular space-occupying lesions, ultrasonography has also been used to assess the status of the fetal cardiovascular system (10). A cystic brain lesion always requires Doppler evaluation to differentiate from other brain cysts. In our patient, two previous ultrasound examinations were normal and this abnormality was detected in 36th week of gestation when the patient was referred for an unrelated problem.
The differential diagnosis includes conditions such as cavum vergae, arachnoid cyst, and porencephalic cyst. All these entities do not show flow on color Doppler imaging (11).
VOGA may be associated with congenital cardiac defects such as sinus venosus, atrial septal defect, coarctation of aorta, partial anomalous pulmonary venous return, patent foramen ovale, ventricular septal defects and atrioventricular canal defects. (12-13).
Contrast enhanced axial CT scan or MRI of the brain usually demonstrates a well-defined, multi-lobulated, intensely enhancing lesion, located within the cistern of velum interpositum. Dilatation of the ventricular system, periventricular white matter hypodensities, as well as diffuse cerebral atrophy are the commonly associated findings. The presence of thrombosis within the aneurysmal sac can be demonstrated well on CT. The thrombus within the aneurysmal sac commonly appears as mixed hypodense, isodense and hyperdense areas due to variable maturation of the clot. On contrast enhanced CT, the presence of a central thrombus and peripheral circulating blood along the wall of the sac can produce the so-called 'Target sign' (14-16). The position and identity of major arterial trunks, primary branches as well as secondary branches feeding the fistula are better identified on MRI than on CT. MR angiography is being increasingly used as a non-invasive alternative to diagnostic angiographic studies in the initial evaluation of these lesions (15-16).
Angiography remains the gold standard for the evaluation of VOGMs. It scores over non-invasive modalities such as CT angiography and MR angiography in demonstrating small feeders supplying the fistula, as well as the dynamic aspects of the venous drainage of the normal brain, and hemodynamic relationships with the venous drainage of the arteriovenous shunt (15-16).
VOGMs are associated with several arterial and venous anomalies. These anomalies represent the persistence of embryological vascular patterns. The limbic ring represents a persistent arterial bridge between the anterior cerebral and anterior choroidal artery. The absence or interruption of the straight sinus is a common association with these anomalies. Persistence of venous channels such as the falcine sinus, occipital sinus and marginal sinus may also be seen. Atresia of transverse and sigmoid sinuses may also be associated.
This malformation is an entity which is known to regress spontaneously at times. It has been documented that Galenic aneurysm with low flow states thrombose and regress with time. (17). Various treatment options are available for patients which include embolisation and surgical correction. The prognosis also depends on the stage at which the patient presents. The earlier the patient presents with symptoms, the worse is the prognosis. Children usually present with high output cardiac failure. The child in our case report was normal at birth with normal respiratory and cardiac parameters.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Kothari SS, Naik N, Juneja R, Saxena A. Aneurysm of the Vein of Galen in neonates: Report of Four Cases. Ind Heart J 2001;53:499-502. [PubMed]
- Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: Embryonic and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989;31:109-28. [CrossRef]
- Wolfgang Dahnert. Brain disorders. In: Radiology review manual. 5th edition. Lippincott Williams and Wilkins, Phoenix, AZ 2002;326-327.
- Cumming GR. Circulation in neonates with intracranial arteriovenous fistula and cardiac failure. Am J Cardiol 1980;45:1019-24. [CrossRef]
- Yasargil MG. Microneurosurgery IIIB. New York: Thieme Medical Publishers; 1988. pp. 323-57.
- Vintzileos AM, Eisenfeld LI, Campbell WA, Herson VC, DiLeo PE, Chameides L. Prenatal ultrasonic diagnosis of arteriovenous malformation of the vein of Galen. Am J Perinatol 1986;3:209-11. [CrossRef]
- Mendelson DB, Hertzanu Y, Butterworth A. In utero diagnosis of a vein of Galen aneurysm by ultrasound. Neuroradiology 1984;26:417-18. [CrossRef]
- Reiter AA, Huhta JC, Carpenter RJ Jr, Segall GK, Hawkins EP. Prenatal diagnosis of arteriovenous malformation of the vein of Galen. JCU 1986;14:623-8. [CrossRef]
- Hirsch JH, Cyr D, Eberhardt H, Zunkel D. Ultrasonographic diagnosis of an aneurysm of the vein of Galen in utero by duplex scanning. J Ultrasound Med 1983;2:231-3. [CrossRef]
- Jeanty P, Kepple D, Roussis P, Shah D. In utero detection of cardiac failure from an aneurysm of the vein of Galen. Am J Obstet Gynecol 1990;163:50-1. [CrossRef]
- Balakumar K. Antenatal Diagnosis of Vein of Galen Aneurysm- Case report. Ind J Radiol Imag 2003;13:91-92.
- Friedman DM, Rutkowski M, Madrid M, Bernstein A. Sinus venosus atrial septal defect associated with vein of Galen malformations: Report of two cases. Pediatr Cardiol 1994;15:50-2. [CrossRef] [PubMed]
- Mc Elhinney DB, Halbach VV, Silverman NH, Dowd CF, Hanley FL.Congenital cardiac anomalies with vein of Galen malformations in infants.Arch Dis Child 1998;78:548-51. [CrossRef]
- Crawford JM, Rossitch E Jr, Oakes WJ, Alexander E 3rd. Arteriovenous malformation of the great vein of Galen associated with patent ductus arteriosus. Childs Nerv Syst 1990;6:18-22. [CrossRef] [PubMed]
- Seidenwurm D, Berenstein A, Hyman A. Vein of Galen malformation: Correlation of clinical presentation, arteriography and MR imaging. AJNR Am J Neuroradiol 1991;12:347-54. [PubMed]
- Horowitz MB, Jungreis CA, Quisling RG, Pollack I. Vein of Galen aneurysms: A review and current perspective. AJNR Am J Neuroradiol 1994;15:1486-96. [PubMed]
- Beltramello A, Perini S, Mazza C. Spontaneously healed vein of Galen aneurysm. Childs Nerv Syst 1991;7:129-34. [CrossRef] [PubMed]
|
| Cite this article as: | | Singh A K, Khetan P K, Srivastava C, Dua S, Gupta V, Dokania S, Bundela Y P, Agarwal V. Pre and Postnatal Diagnosis of Vein of Galen Aneurysm- A Case Report. Pediatr Oncall J. 2008;5: 83. |
|