|
Subcutaneous Emphysema and Spontaneous Pneumomediastinum in a Toddler
Sudhir Kumar Rana, Ragini Singh, Chhavi S Nanda.
Department of Pediatrics, SGRRIM and HS, Dehradun, India.
ADDRESS FOR CORRESPONDENCE
Dr Sudhir Kumar Rana, Department of Pediatrics, SGRRIM & HS, Dehradun, India. 248001.
Email: drsudhirrana@gmail.com

|
|
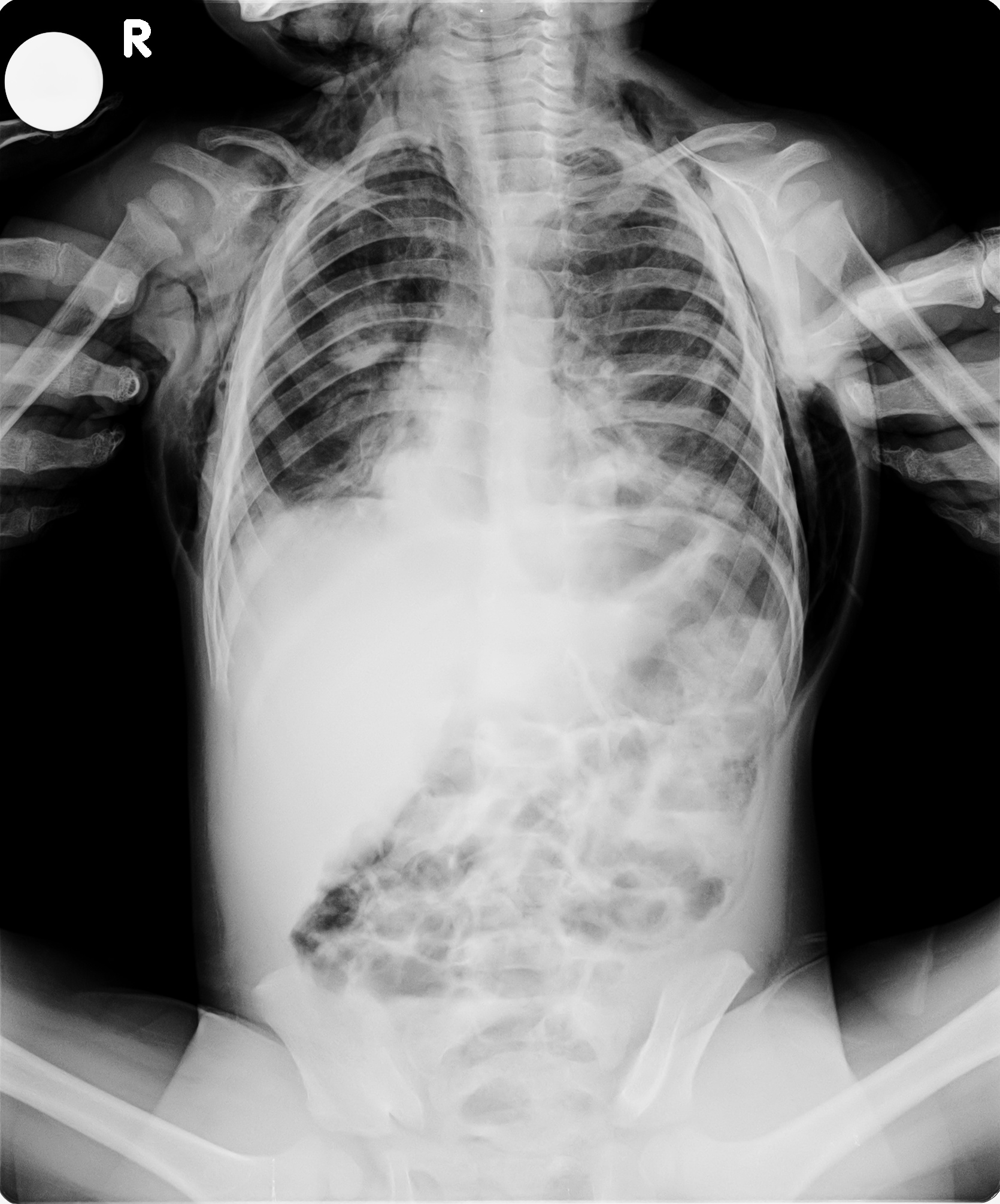
What is the diagnosis?
Hamman syndrome {Macklin`s syndrome} consists of spontaneous subcutaneous emphysema {SCE} and spontaneous pneumomediastinum {SPM}, without pneumothorax. It is rarely reported in young children. Incidence of SPM is around 3 per 1000 children presenting with asthma. {1} Causes of Hamman syndrome are {a} valsalva maneuvers, {b} severe broncho-pulmonary infections, asthma, and pandemic {H1N1} influenza, {c} foreign body ingestion, {d} Boerhaave syndrome and {e} Thoracic or dental surgery. Very often etiology remains unknown. {2} It is easily confused with potentially lethal Boerhaave syndrome which is spontaneous rupture of the esophagus after vomiting. Clinical presentation include sudden onset of cough, SCE, remarkable chest pain, sore throat, voice change, odynophagia, swelling of the neck, pain in neck, chest , dysphagia, dyspnea, respiratory distress and air leak to parts of the trunk and limbs. Diagnosis is confirmed by X-ray chest PA and lateral view {2} showing air streaks outlining mediastinal structures, especially around cardiac landmarks. Serial X-rays are not recommended. CT chest is considered the gold standard for diagnosis of SPM and while contrast CT chest may be needed in Boerhaave syndrome on suspicion of esophageal rupture and mediastinitis. {2} Conservative management and treatment of primary cause are the mainstay of treatment of Hamman syndrome. However in presence of severe respiratory distress, measures like multiple skin incisions at the level of thoracic inlet, placement of subcutaneous drain and high flow oxygen therapy are employed. {2}
Funding: Nil
Acknowledgement: Nil
Conflict of interest: Nil |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Bullaro FM, Bartoletti SC. Spontaneous pneumomediastinum in children: a literature review. Pediatr Emerg Care. 2007; 23: 28–30. [CrossRef] [PubMed]
- Caceres M, Ali SZ, Braud R, Weiman D, Garrett HE Jr. Spontaneous pneumomediastinum: a comparative study and review of the literature. Ann Thorac Surg. 2008; 86: 962–966 [CrossRef] [PubMed]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2014.18 |
| |
Cite this article as:
Rana S K, Singh R, Nanda C S. Subcutaneous Emphysema and Spontaneous Pneumomediastinum in a Toddler (Hamman Syndrome). Pediatr Oncall J. 2014;11: 57. doi: 10.7199/ped.oncall.2014.18
|