|
Incessant vomiting
Girish Gopal, Keerthan G, Veeresh H, Sudha Rudrappa.
Department of Pediatrics, Mysore Medical College and Research Institute, Mysore, Karnataka, India.
ADDRESS FOR CORRESPONDENCE
Dr. Girish Gopal, Senior Resident, Department of Pediatrics, Mysore Medical College and Research Institute, Irwin Road, Mysore – 570021, Karnataka, India.
Email: girishgpl@gmail.com
|
|
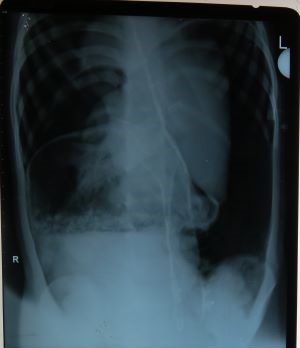
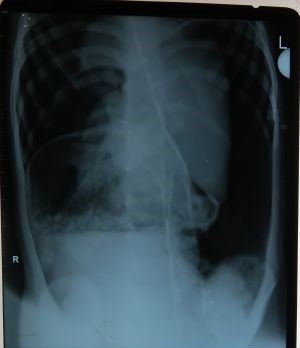
What is the diagnosis?
A working diagnosis of acute gastric volvulus was made and she was taken up for emergency laparotomy during which a combined organoaxial and mesentericoaxial type of gastric volvulus with necrosis of the perforated stomach and entire spleen was seen. She underwent near-total gastrectomy and splenectomy. Despite the surgery her hemodynamics didn’t improve and she succumbed on the second post-operative day.
Gastric volvulus is a significant, rare cause of non-bilious vomiting and consists of pathological rotation of the stomach of more than 180 degree around the axis, creating a closed loop obstruction that can result in incarceration and strangulation. {1} It was first described by Berti in 1866. {1} Males and females are equally affected. Gastric volvulus in children is often secondary to congenital diaphragmatic defects. {1} Singleton classified gastric volvulus based on the axis around which the stomach rotates and includes organoaxial {59 percent of cases, the stomach rotates around an axis that connects the gastroesophageal junction and pylorus}, mesentericoaxial {29 percent of cases, stomach rotates around an axis joining the lesser and greater curvature} and combined type {12 percent of cases, stomach rotates around both axes}. {2} Gastric volvulus can be idiopathic {Type 1} or due to congenital or acquired causes {Type 2}. Type 1 comprises two thirds of the cases and is presumably due to abnormal laxity of gastrosplenic, gastroduodenal, gastrophrenic and gastrohepatic ligaments. Type 2 is found in one third of the cases and is more common in children. It is often secondary to congenital or acquired defects in the diaphragm. {3} Clinical symptoms depend upon the extent or degree of rotation, obstruction and associated defects. The Borchardt triad of abdominal pain, retching and inability to pass a nasogastric tube is diagnostic of acute volvulus and occurs in 70 percent of cases. {3} Our case had this classical triad. Intermittent epigastric pain, dyspepsia, dysphagia, dyspnea and failure to thrive are seen in cases with chronic volvulus. Diagnosis can be confirmed by radiography {plain film and barium contrast} or computed tomography. Plain radiography may reveal massively distended viscus, paucity of distal gas shadow with or without air fluid levels and pneumoperitoneum. {4} Surgical repair is the treatment of choice. Surgical options include, simple gastropexy, gastropexy with division of the gastrocolic omentum, partial gastrectomy, fundoantaral gastrogastrostomy, and repair of diaphragmatic hernia or eventration if present. {5} Non-operative mortality rate for gastric volvulus is as high as 80 percent, the major cause of death being strangulation which can lead to necrosis and perforation as in our case. With early diagnosis and good surgical management the mortality rates has decreased to 15-20 percent in acute volvulus and 0-13 percent in chronic volvulus. {6}
Conflict of Interest: None
Funding: None |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Porcaro F, Mattioli G, Romano C. Pediatric gastric volvulus: Diagnostic and Clinical Approach. Case Rep Gastroenterol 2013; 7: 63-68. [CrossRef] [PubMed] [PMC free article]
- Singleton AC. Chronic gastric volvulus. Radiology 1940; 34: 53-61. [CrossRef]
- Miller DL, Pasquale MD, Seneca RP, Hodin E. Gastric volvulus in the pediatric population. Arch Surg. Sep 1991; 126: 1146-1149. [CrossRef] [PubMed]
- Woo-Hyun Park, Soon-Ok Choi, Soo-Jhi Suh. Pediatric Gastric Volvulus. Journal of Korean Medical Sciences 1992; 7: 258-263. [CrossRef] [PubMed] [PMC free article]
- Tanner NC. Chronic and recurrent volvulus of the stomach with late results of colonic displacement. Am J Surg 1968; 115: 505-515 [CrossRef]
- Palanivelu C, Rangarajan M, Shetty AR, Senthilkumar R. Laparoscopic suture gastropexy for gastric volvulus: a report of 14 cases. Surg Endosc 2007; 21: 863-866. [CrossRef] [PubMed]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2014.59 |
| |
Cite this article as:
Gopal G, G K, H V, Rudrappa S. Incessant vomiting (Acute Gastric Volvulus). Pediatr Oncall J. 2014;11: 126-127. doi: 10.7199/ped.oncall.2014.59
|