Girish Gopal1, Gangadhar B Belavadi2.
1Department of Pediatrics, Mysore Medical College and Research Institute, Mysore, India,
2Department of Pediatrics, Bangalore Medical College and Research Institute, Bangalore, India.
ADDRESS FOR CORRESPONDENCE
Dr. Girish Gopal, Senior Resident, Department of Pediatrics, Mysore Medical College and Research Institute, Irwin Road, Mysore – 570021, Karnataka, India.
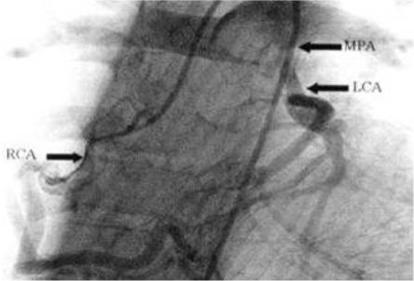
Email: girishgpl@gmail.com | | Keywords | | ALCAPA, congenital anomaly, congestive cardiac failure, myocardial infarction, sudden cardiac death. | | | A 9 month old male infant presented with cough, increased irritability, hurried breathing, chest in-drawing, interrupted feeding and diaphoresis for four days prior to admission. He had regular doctor visits from early infancy for recurrent upper respiratory tract infections, episodes of inconsolable crying, and poor weight gain for which he had received multiple oral antibiotics, nasal decongestants, antitussives, antispasmodics and hematinics but with no significant improvement in these symptoms. On presentation this time, he appeared sick, irritable, had severe pallor, periorbital puffiness and sacral edema with tachypnea (respiratory rate – 76/min) and tachycardia (heart rate-184/min). He was hyperglycemic (random blood sugar was 246mg/dl), severely underweight (4.2kgs) and stunted (58cms). His peripheries were cold with poor pulses and prolonged capillary refill time (CRT) of > 3sec. Oxygen saturation with 6 litres of oxygen varied between 95-98%. He had precordial bulge with pushed down heaving apical impulse and S3 gallop on auscultation. Crackles were heard at the basal areas of lung fields and there was tender hepatomegaly. He was treated with oxygen, empirical antibiotics, intravenous fluids (restricted maintenance), dobutamine at 10 µg/kg/min, digoxin, diuretics and packed red cell transfusion in view of hemoglobin being 4.4 g/dl. Chest x-ray revealed pulmonary plethora and massive cardiomegaly with left ventricular type of apex and cardiothoracic ratio of 0.72. Electrocardiograph showed left ventricular (LV) enlargement and Q waves in lead I and avL. Colour doppler echocardiography showed concentric left ventricular hypertrophy with ejection fraction of around 60% and origin of the left main coronary artery (LCA) from the main pulmonary trunk with reversal of flow in the LCA. Coronary angiogram confirmed the diagnosis of anomalous origin of the left main coronary artery (ALCAPA). (Figure 1) The child underwent an uncomplicated aortic reimplantation of the LCA and his recurrent symptoms abated.
Figure 1: Coronary angiogram of the child showing origin of the LCA from the main pulmonary artery.
The anomalous origin of LCA from the pulmonary artery (PA) is a rare but serious congenital cardiac anomaly accounting for approximately 0.25%-0.5% of all congenital heart diseases. (1) The first clinical description was described by Edward Bland, Paul Dudley White and Joseph Garland in 1933; hence it is also known as Bland-White-Garland syndrome. (2) It occurs equally in both males and females and is not considered an inheritable congenital cardiac defect. Embryologically, this anomaly arises from either abnormal septation of the conotruncus into the aorta and pulmonary artery, or from persistence of the pulmonary buds together with involution of the aortic buds that eventually form the coronary arteries. (3) In fetal and early neonatal life, ALCAPA is well tolerated. After birth the pulmonary arterial pressure drops. Collateral circulation between the right and left coronary artery ensues and with further decrease in pulmonary arterial pressure there is reversal of flow, as the LCA drains from RCA through collaterals, into the pulmonary artery. This is known as the coronary steal phenomenon and causes ischemia and infarction of the anterolateral left ventricular wall and mitral valve papillary muscle dysfunction causing variable degrees of mitral valve insufficiency. (4) Spectrum of clinical presentation includes sudden death in infancy to asymptomatic survival into adulthood. With progressive ischemia of the left ventricle (LV) and increase in the severity of mitral insufficiency, signs and symptoms of congestive cardiac failure (CCF) ensue, leading to poor weight gain. Chest radiograph may show significant cardiomegaly with or without pulmonary plethora. Electrocardiograph may show left ventricular enlargement, left axis deviation and Q waves in leads I, avL and V4-V6. Colour doppler echocardiography is often diagnostic of ALCAPA. In most cases, it identifies the anomalous origin of LCA and also the color flow velocity mapping demonstrates the retrograde flow from the anomalous LCA into the pulmonary trunk. Variable degrees of mitral valve regurgitation, left ventricular dysfunction, and regional wall motion abnormalities may also be identified. Cardiac catheterization with angiography, CT angiography, and MR angiography are the other diagnostic tests. (5) Medical management of ALCAPA includes the use of diuretics, ACE inhibitors and inotropic agents during CCF. Once the symptoms of CCF are controlled, surgical correction remains the mainstay of treatment. Surgical procedures include (i) a left subclavian – coronary artery anastomosis (ii) a saphenous vein bypass graft (iii) Takeuchi procedure (creation of an aortopulmonary window and an intrapulmonary tunnel extending from the anomalous ostium to the window and (iv) direct reimplantation of the anomalous LCA to the aorta. (6) Mortality rate is 90% for infants with surgically uncorrected ALCAPA. (5) However, children undergoing successful surgical correction have favorable prognosis and good long-term survival. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Menahemm S, Venables AW. Anomalous left artery from the pulmonary artery: a 15 year sample. Br Heart J 1987; 58: 78-84. [CrossRef]
- Bland EF. Congenital anomalies of the coronary arteries: report of an unusual case associated with cardiac hypertrophy. Am Heart J 1933; 8: 787-801. [CrossRef]
- Lardhi AA. Anomalous origin of left coronary artery from pulmonary artery: A rare cause of myocardial infarction in children. J Fam Community Med 2010; 17: 113-116. [CrossRef]
- Cowles RA, Berdon WE. Bland-White-Garland syndrome of anomalous left coronary artery arising from the pulmonary artery: A historical review. Pediatr Radiol 2007; 37: 890-895. [CrossRef]
- Pena E, Nquyen Merchant N, Dennie G. ALCAPA syndrome: Not just a pediatric disease. Radio-graphics 2009; 2: 553-565. [CrossRef]
- Erdinc M, Hosgor K, Karahan O. Repair of anomalous origin of the left coronary artery arising from right pulmonary artery with rolled-conduit-extended reimplantation in an adult. J Card Surg 2011; 26: 604-607 [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2014.63
|
| Cite this article as: | | Gopal G, Belavadi G B. Anomalous Origin of the Left Main Coronary Artery (ALCAPA) Syndrome Masquerading as Severe Anemia in Infancy. Pediatr Oncall J. 2014;11: 118-119. doi: 10.7199/ped.oncall.2014.63 |
|