|
UNILATERAL CYSTIC LUNG LESIONS
Vivek Sharma, Amalendu Das, Venkat Reddy, Smriti Nath.
Department of Pediatrics, Tata Motors Hospital, Jamshedpur, Jharkhand, India.
ADDRESS FOR CORRESPONDENCE
Dr Vivek Sharma, M-36, 4, Telco colony, Jamshedpur, Jharkhand – 831004, India.
Email: dr_viveksharma@yahoo.com

|
|
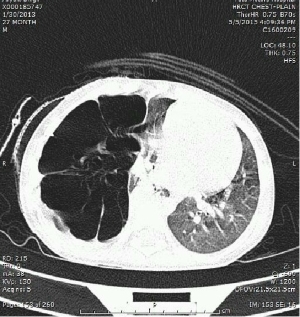
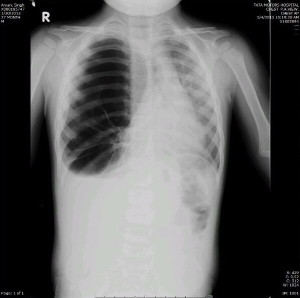
What is the diagnosis?
Congenital Cystic Adenomatoid Malformation {CCAM}. CCAM is rare abnormality of lung development and a multicystic mass of segmental lung tissue with abnormal bronchial proliferation. {1} Incidence ranges from 1 in 11,000 to 1 in 35,000. {2,3} Lesions are usually unilateral and involve single lobe. Currently CCAM is classified into five types {Type - 0 to Type - 4} based on origin and histological features. {4,5} Type-0 is the rarest form and arises from trachea or bronchus. Type-1 is the most common form and arises from distal bronchus or proximal bronchus which is usually macrocystic. Type-2 arises from terminal bronchioles, usually microcystic and associated with other congenital anomalies. Type-3 arises from acinar-like tissue. Type-4 is generally associated with malignancy. Type-1 has good prognosis whereas Type-0 is lethal. Diagnosis can be done in antenatal period by ultrasonography. In postnatal period diagnosis can be done by plain x-ray chest which shows expansile soft tissue mass containing multiple air-filled cystic masses of varying sizes and shifting of mediastinum. CT scan confirms the diagnosis and helps in the classification of the condition. Surgical resection of CCAM is the mainstay of treatment. {1} |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Sfakianaki AK, Copel JA. Congenital Cystic Lesions of the Lung: Congenital Cystic Adenomatoid Malformation and Bronchopulmonary Sequestration. Rev Obstet Gynecol. 2012;5:85–93 [PubMed] [PMC free article]
- Laberge JM, Flageole H, Pugash D, Khalife S, Blair G, Filiatrault D, et al. Outcome of the prenatally diagnosed congenital cystic adenomatoid lung malformation: a Canadian experience. Fetal Diagn Ther. 2001;16:178–86. [CrossRef] [PubMed]
- Gornall AS, Budd JL, Draper ES, Konje JC, Kurinczuk JJ. Congenital cystic adenomatoid malformation: accuracy of prenatal diagnosis, prevalence and outcome in a general population. Prenat Diagn. 2003;23:997–1002. [CrossRef] [PubMed]
- Stocker JT, Madewell JE, Drake RM. Congenital cystic adenomatoid malformation of the lung. Classification and morphologic spectrum. Hum Pathol. 1977;8:155–71. [CrossRef]
- Stocker JT. Cystic lung disease in infants and children. Fetal Pediatr Pathol. 2009;28:155–184. [CrossRef] [PubMed]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2015.63 |
| |
Cite this article as:
Sharma V, Das A, Reddy V, Nath S. UNILATERAL CYSTIC LUNG LESIONS. Pediatr Oncall J. 2015;12: 118. doi: 10.7199/ped.oncall.2015.63
|