Sarath Balaji B, Kalpana S, Selladurai Elilarasi, Sundari S.
Department of Pediatric Pulmonology, Institute of Child Health and Hospital for Children, Egmore, Chennai, Tamilnadu, India.
ADDRESS FOR CORRESPONDENCE
Dr Kalpana Sivasambo, Department of Pediatric Pulmonology, Institute of Child Health and Hospital for Children, Egmore, Chennai, Tamilnadu, India
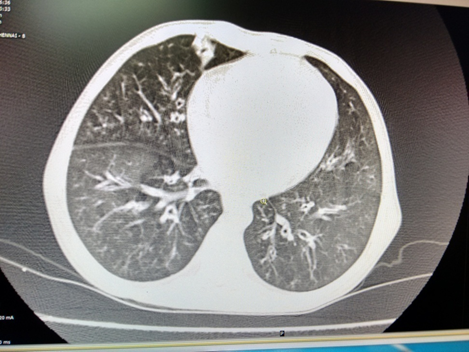
Email: drskalpana@yahoo.co.in | | Abstract | | Atypical presentations of celiac disease are well recognised but respiratory symptoms as a manifestation are rare. A 6 years old girl presented with recurrent respiratory tract infections and bronchiectasis along with intermittent altered bowel habits. Serology, duodenal biopsy and bronchoalveolar lavage showing lymphocytic bronchoalveolitis narrowed the diagnosis to celiac disease. Dramatic improvement was observed in both the respiratory and gastrointestinal manifestations following gluten free diet. | | | | Keywords | | celiac, respiratory, atypical manifestation | | | | Introduction | | Celiac disease is not an uncommon condition in northern India where the estimated prevalence is about 1 in 96, but still remains a rare or underdiagnosed entity in the Southern parts. (1,2) Though the typical manifestations such as chronic or recurrent diarrhea, anemia and short stature are well recognised, the atypical symptoms can be quite misleading. We report a case of celiac disease with predominant pulmonary manifestation as a presenting complaint. | | | | Case Report | A 6 years old girl born of second degree consanguineous parents, hailing from Andhra Pradesh was referred to us for evaluation of recurrent respiratory tract symptoms (cough with on and off breathing difficulty) since 6 months of age. The mother also gave history of recurrent diarrhea, abdominal distension and failure to thrive noticed from 4 years of age. There were previous hospitalisations thrice for pneumonia like illnesses which were managed with intravenous antibiotics. The child had also received a course of empirical antituberculous drugs at 5 years of age in view of her recurrent respiratory symptoms. On examination, she was apathetic with severe thinness (both her weight and height were less than the 3rd centile for age), had pallor and pan-digital clubbing. She also had conjuctival xerosis, glossitis and stomatitis. Her oxygen saturation was 97% in room air with stable vital parameters though respiratory rate was 40/min. There were bilateral crepitations all over the lung fields. Other systems were normal. On investigations she had microcytic anemia (hemoglobin: 8.8 gm%), total and differential white cell counts were normal. Renal and liver function tests were within normal limits. Ultrasonogram (USG) of abdomen did not reveal any abnormalities. Chest xray showed bilateral diffuse infiltrates and a subsequent HRCT chest showed bronchiectatic changes bilaterally (Figure 1). Sweat chloride by pilocarpine iontophoresis was 4 meq (Normal <60 meq). Immunoglobulin profile, flow cytometry and nitroblue tetrazolium test were normal. Mantoux test and induced sputum for GenXpert for mycobacterium tuberculosis were negative. Bronchoalveolar lavage (BAL) for aerobic, fungal and tuberculosis culture did not grow any organism. The cytology showed a predominant lymphocytic (20%) inflammation; 74% alveolar macrophages, 2% neutrophils and 4% eosinophils. In view of associated diarrhea, pallor and short stature a diagnosis of celiac disease was considered. Serum IgA tissue transglutaminase was increased [105.2 (normal: ≤10 IU/L)]. A subsequent duodenal biopsy demonstrated villous atrophy with increase in intraepithelial lymphocytes. A final diagnosis of celiac disease with respiratory involvement was made.
Following institution of a gluten free diet, the child showed overall improvement in her condition including decrease in frequency of respiratory and gastrointestinal symptoms in addition to the improvement observed in her growth. The bilateral lung signs disappeared and the chest xray which had shown persistent diffuse infiltrates also became normal. A repeat CT chest was however deferred. During follow-up, with accidental ingestion of gluten containing chocolates, the child presented with reappearance of lung crepitations and respiratory distress which improved after stopping the offending diet.
Figure 1: HRCT chest showing bilateral bronchiectatic changes
| | | | Discussion | | Classical symptoms of celiac disease like chronic or intermittent diarrhea, failure to thrive, weight loss, stunted growth, delayed puberty, amenorrhoea and iron-deficiency anemia usually prompt an early evaluation especially in geographic areas where celiac disease is prevalent. Our patient presented with recurrent respiratory tract infection with early bronchiectasis along with the classical features like intermittent diarrhea, failure to thrive and anemia. A similar presentation has been described by Kallel-Sellami et al in an adult with recurrent pulmonary infections and intermittent intestinal symptoms in childhood, who was subsequently diagnosed with celiac disease. (3) bal cytology in our patient demonstrated a predominant lymphocytic bronchial inflammation. Brightling et al have reported an identical case of cough, lymphocytic bronchoalveolitis and celiac disease with improvement following a gluten free diet. (4) Our case also demonstrated a dramatic improvement in all her symptoms on stopping gluten in the diet. An association between celiac disease and obstructive airway symptoms like asthma and chronic cough was also demonstrated by Tarlo et al. (5) A number of other pulmonary complications including diffuse pulmonary nodules, interstitial fibrosis, bronchiectasis and alveolitis have been linked to coeliac disease. (6,7) The cause of the association of pulmonary disorders with coeliac disease remains poorly defined. Absorption of an extrinsic allergen or immune complexes through an abnormal gastrointestinal mucosa may lead to the pulmonary disease. (8) Alternatively, the association of celiac disease with HLA status and various autoimmune diseases suggests that a common disturbance in immunity may underlie both celiac disease and pulmonary disorders. | | | | Conclusion | | Celiac disease must be considered as a possible etiology of chronic respiratory symptoms even in less prevalent geographic areas as a gluten free diet produces a dramatic response in the children’s clinical condition. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Makharia GK, Verma AK, Amarchand R, Bhatnagar S, Das P, Goswami A et al. Prevalence of celiac disease in the northern part of India: a community based study. J Gastroenterol Hepatol. 2011;26(5):894-900. [CrossRef] [PubMed]
- Ganesh R, Suresh N, Sathiyasekaran M. Celiac disease, still an uncommon problem in Tamilians? Ind J Gastroenterol 2009:28(5):189–19. [CrossRef] [PubMed]
- Kallel-Sellami M, Laadhar L, Zitouni M, Makni S.Recurrent rhinitis and pulmonary infections revealing celiac disease: case report. Rev Pneumol Clin. 2008; 64(1):27-9. [CrossRef] [PubMed]
- Brightling CE, Symon FA, Birring SS, Wardlaw AJ, Robinson R, Pavord ID. A case of cough, lymphocytic bronchoalveolitis and celiac disease with improvement following a gluten free diet. Thorax 2002; 57:91-92. [CrossRef] [PubMed]
- Tarlo SM, Broder I, Prokipchuk EJ, Peress L, Mintz S. Association between celiac disease and lung disease. Chest 1981; 80:715-8. [CrossRef] [PubMed]
- Edwards C, Williams A, Asquith P. Bronchopulmonary disease in coeliac patients. J Clin Pathol. 1985;38:361–367. [CrossRef] [PubMed]
- Wallaert B, Prin L, Hatron PY, Ramon P, Tonnel AB, Voicin C. Lymphocyte subpopulations in bronchoalveolar lavage in Sjogren's syndrome. Evidence for an expansion of cytotoxic/suppressor subset in patients with alveolar neutrophilia. Chest. 1987; 92:1025–31. [CrossRef] [PubMed]
- Hood J, Mason AMS. Diffuse pulmonary disease with transfer factor defect occurring with coeliac disease. Lancet 1970; 1 (7644):445–448. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2016.20
|
| Cite this article as: | | B S B, S K, Elilarasi S, S S. Respiratory Symptoms as Atypical Manifestation of Celiac Disease. Pediatr Oncall J. 2016;13: 46-47. doi: 10.7199/ped.oncall.2016.20 |
|